Accessible Health Care Briefs: HEALTH CARE (Clinic/Outpatient) FACILITIES ACCESS
HEALTH CARE (Clinic/Outpatient) FACILITIES ACCESS
June Isaacson Kailes MSW, Associate Director
Christie Mac Donald MPP, Senior Policy Analyst
Center for Disabilities Issues and the Health Professions
Western University of Health Sciences
309 E. Second Street, Pomona, CA 91766
Voice909.469.5213/
TTY909.469.5520,
Fax 909.469.5503
ahcs@westernu.edu
Edition 2: Updated 01.05.09
This brief is part of the Accessible Health Care Series available at
www.cdihp.org/products.html#access_briefs
Distribution is encouraged, and permission is granted provided that:
(1) This copyright notice and citation is attached to each copy;
Kailes, J., and Mac Donald, C., Health Care (Outpatient / Clinic) Facilities Access, 2009. Published and distributed by the Center for Disability Issues and the Health Profession, Western University of Health Sciences, 309 E. Second Street, Pomona, CA 917661854, Voice909.469.5213/ TTY909.469.5520, available at www.cdihp.org/products, Email: ahcs@westernu.edu
(2) No alterations are made to the contents of the document;
(3) The document is not sold for profit; and
(4) The Center for Disability Issues and the Health Professions is notified of such use.
Edition 1 of this brief was funded, in-part, by the National Institute on Disability and Rehabilitation Research, U.S. Department of Education, under grant #H133E020729. The Rehabilitation Engineering Research Center (RERC) on Accessible Medical Instrumentation was a five-year project that evaluates methods and technologies to increase the accessibility and usability of diagnostic, therapeutic, and procedural healthcare equipment, and associated assistive technologies, for people with disabilities.
1. a. Complying with the ADA
The major pieces of federal legislation governing equal access to health care services for individuals with disabilities are the Rehabilitation Act (Rehab Act) and the Americans with Disabilities Act (ADA). These laws constitute a national mandate prohibiting discrimination based on disability in the provision of goods and services available to the public.
Section 504 of the Rehab Act prohibits any organization that receives federal financial assistance from denying individuals with disabilities equal access to the services. For example, hospitals, clinics, and other health care facilities that accept Medicaid, Medicare, or any other form of federal funding must comply with the Rehab Act. Section 504 states, “No otherwise qualified individual with a disability . . . shall, solely by reason of her or his disability, be excluded from the participation in, be denied the benefits of, or be subjected to discrimination under any program or activity receiving federal financial assistance.” If the provider serves just one Medicare or Medicaid beneficiary, that provider’s entire operations must comply with the Rehab Act. Medicare and Medicaid managed care plans must provide programmatic access to all its enrollees with disabilities.i
ADA’s Title II extends the Rehab Act’s requirements to all state and local government activities. All health care providers who offer health care services, either directly or through contractual arrangements, to Medicare or Medicaid beneficiaries must comply with the Rehab Act because Medicare and Medicaid funding is considered federal financial assistance.ii
ADA’s Title III states: “No individual shall be discriminated against on the basis of disability in the full and equal enjoyment of the goods, services, facilities, privileges advantages, or accommodations of any place of public accommodation by any person who owns, leases (or leases to), or operates a place of public accommodation.”
All health care providers, including hospitals, nursing homes, psychiatric and psychological services, private physicians’ offices, diagnostic centers, physical therapy centers, and health clinics, are places of public accommodations and therefore must comply with Title III.iii
1. b. ADA Accessibility Guidelines for Buildings and Facilities (ADAAG)
ADA Accessibility Guidelines for Buildings and Facilities (ADAAG) contains scoping and technical requirements for accessibility to buildings and facilities by individuals with disabilities under the Americans with Disabilities Act (ADA) of 1990. Technical requirements are to be applied during the design, construction, and alteration of buildings and facilities covered by titles II and III of the ADA to the extent required by regulations issued by Federal agencies, including the Department of Justice and the Department of Transportation, under the ADA.iv (See Section 4: Government Resources, page 17 for contact information)
2. IMPROVING PHYSICAL ACCESS
People with disabilities should be able to travel to a health care site, approach and enter and move around the building as conveniently as everyone else. Access issues that should be considered include:
2. a. Accessible route into and throughout the facility - The following is a 4-point guideline for ensuring equal access from the parking lot, outdoor walkways, entrances and exists of the buildings.
-
At least one accessible route within the boundary of the site shall be provided from public transportation stops, accessible parking, and accessible passenger loading zones, and public streets or sidewalks to the accessible building entrance they serve. The accessible route shall, to the maximum extent feasible, coincide with the route for the general public.
-
At least one accessible route shall connect accessible buildings, facilities, elements, and spaces that are on the same site.
-
At least one accessible route shall connect accessible building or facility entrances with all accessible spaces and elements and with all accessible dwelling units within the building or facility.
-
An accessible route shall connect at least one accessible entrance of each accessible dwelling unit with those exterior and interior spaces and facilities that serve the accessible dwelling unit.v
2. a. i. Accessible Parking vi
“A greater number of accessible parking spaces is required at facilities providing medical care and other services for persons with mobility impairments. The term "mobility impairments" is intended to include:
-
conditions requiring the use or assistance of a brace, cane, crutch, prosthetic device, wheelchair or other mobility aid;
-
arthritic, neurological, or orthopedic conditions that severely limit one's ability to walk;
-
respiratory diseases and other conditions which may require the use of portable oxygen; or
-
cardiac conditions that impose significant functional limitations.
At outpatient facilities, 10% of the parking spaces must be accessible. Facilities that specialize in medical treatment and other services for persons with mobility impairment are required to have 20% of parking spaces accessible. Other facilities (including medical care facilities) that do not provide outpatient services or specialized service for persons with mobility impairments are subject only to the general scoping requirement in the table in ADAAG 4.1.2(5)(a).”
-
Facilities and Units Specializing in Treatment or Services for Persons with Mobility Impairments
“Facilities or units that specialize in treatment or other services for persons with mobility impairments, including vocational rehabilitation and physical therapy, must have 20% of parking spaces accessible. These are facilities in which the treatment or service specifically serves persons with mobility impairments, such as spinal cord injury treatment centers, prosthetic and orthotic retail establishments, and vocational rehabilitation centers for persons with mobility impairments. This requirement does not apply to facilities providing, but not specializing in, services or treatment for persons with mobility impairments, such as general rehabilitative counseling or therapy centers. In determining whether a facility is subject to this requirement, both the nature of the services or treatment provided and the population they serve should be carefully considered.”
Note: for more information on parking and loading specifications including diagrams, slope requirements, location, and signage, refer to ADAAG Section 4.6 Parking and Passenger Loading Zones.
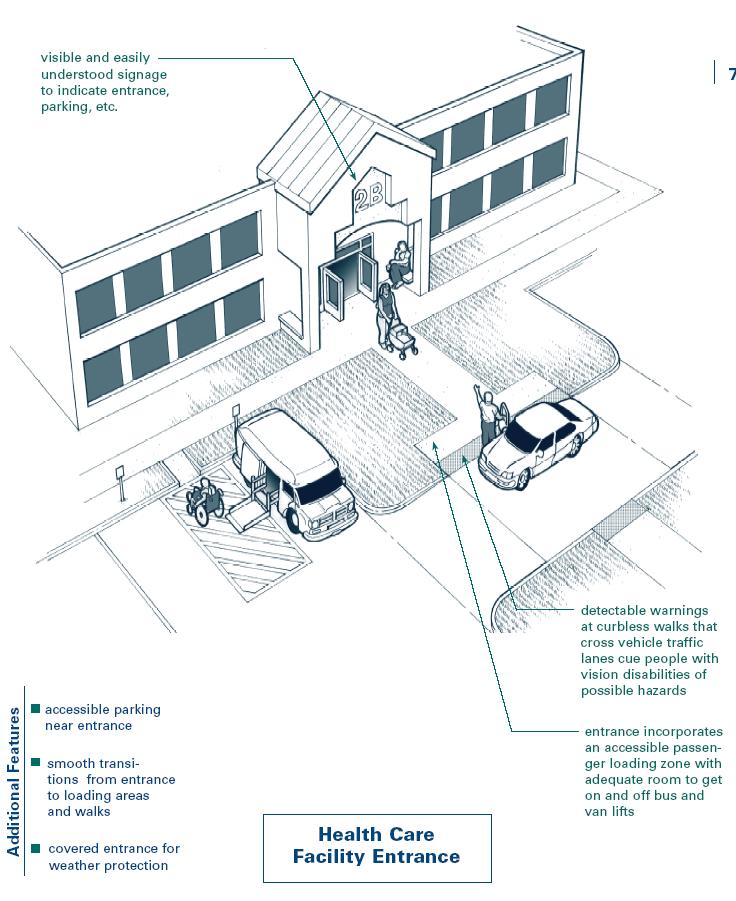
Figure 1: Health care facility entrance depicting accessible parking, smooth transitions to loading and walking areas, covered entrance, and easily visible entrance signage.vii
A. Directional Signage
-
If the accessible entrance is one other than the main entrance, a sign at the main entrance should indicate the location of the accessible entrance and the alternate route for access. The travel distances from the general route need to be minimized.viii Signage may be necessary along routes to avoid confusion.
Figure 2: Direction signage indicating accessible entrance pointing to the right side of the building.
-
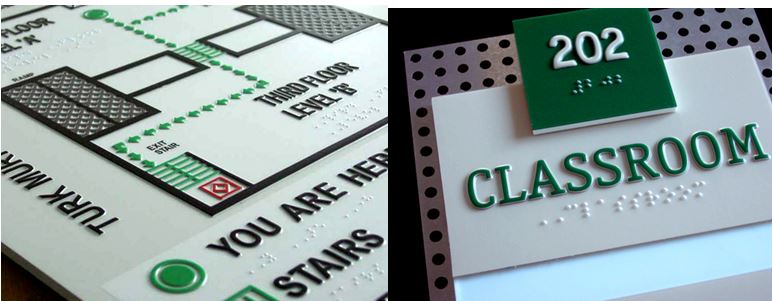
Effective Braille and tactile signs are an important way to make facilities welcoming and functional for people with vision limitations. “Characters and symbols should have backgrounds in eggshell, matte, or other non-glare finish, and contrast with their background -- either light characters on a dark background or dark characters on a light background.” ix
Figure 3 and 4: Two examples of signage containing contrasting colors, tactile diagrams and Braille.x

For a complete list of signage specifications including character height, proportion, font, size, and mounting placement refer to ADAAG Section 4.30 Signage.
2. a. iii. Clear (Path-of-Travel) Floor Space
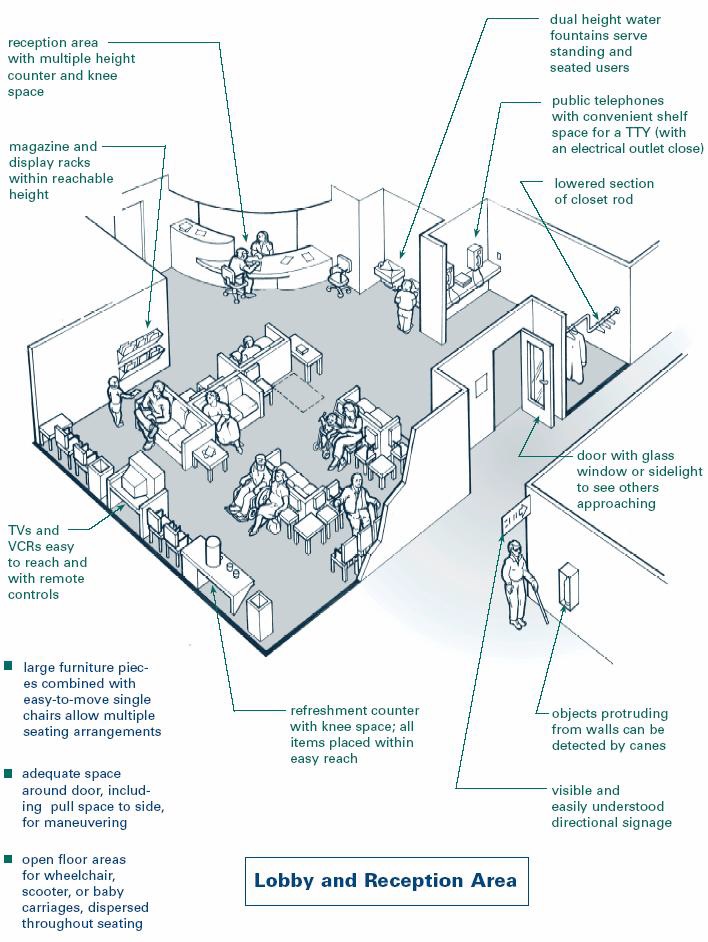
Access also includes how people will move into and around lobby and office reception areas, and determine the unobstructed floor or ground space to accommodate a wheelchair user. (Figure 7 below)xi
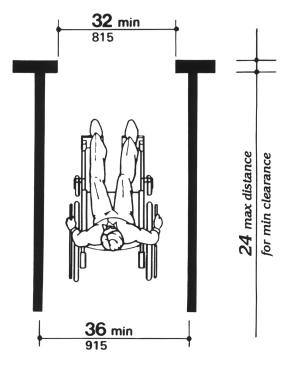
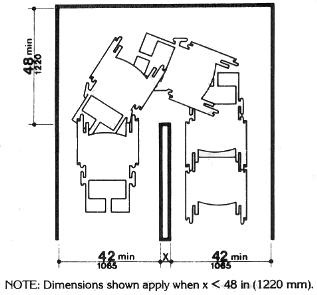
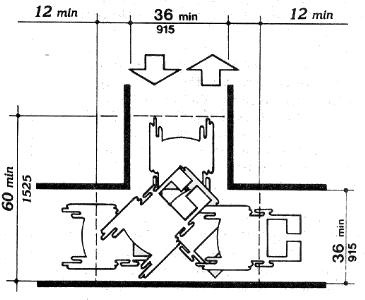
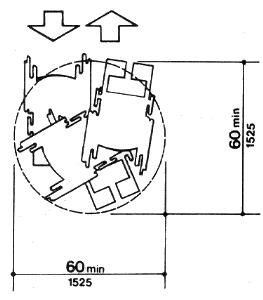
2. a. iv. Path-of-Travel (wheelchair) space allowances.xii In general, a 36” wide accessible route is needed with a slightly larger space provided at corners. If a 180° turn is needed to exit an area, then a 60” diameter turning space or a 36” wide "T" is needed (see Figure 11).
-
C1. Accessible route turns around an obstruction:
-
C2. T-Shaped Space for 180° degree turns
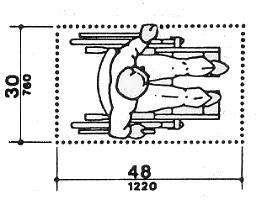
A - Figure 8: Clear ground space width: The minimum clear floor or ground space required accommodating a single, stationary wheelchair and occupant is 30 in by 48 in (760 mm by 1220 mm).
B – Figure 9: Maximum doorway depth and passage width: The minimum clear passage width for a single wheelchair shall be 36 inches (915 mm) minimum along an accessible route, but may be reduced to 32 inches (815 mm) minimum.
C1 – Figure 10: Accessible route turns around an obstruction: A U-turn around an obstruction less than 48 inches (1220 mm) wide may be made if passage width is a minimum of 42 inches (1065 mm) and base of U-turn space is a minimum of 48 inches.
C2 – Figure 11: T-Shaped Space for 180° Degree Turns. The T-shape space is 36 inches (915 mm) wide at the top and stem within a 60-inch-by-60 in.
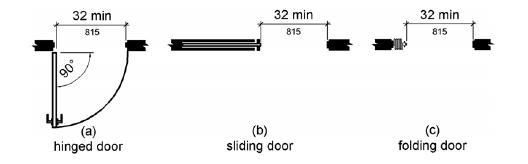
2. b. i. Clear door openings: Door openings should provide a clear width of 32 inches (815 mm) minimum. Clear openings of doorways with swinging doors shall be measured between the face of the door and the stop, with the door open 90° degrees.xiv
Figure 13: Clear width of doorways – 32 inches
2. b. ii. Accessible Door Hardware
-
Door handles: Inaccessible door hardware (Figure 14 below) can prevent access to medical offices. For example, the handle shown below requires the user to tightly grasp the handle to open the door. People who have limitations in grasping, such as arthritis, find this type of handle difficult or impossible to use. Hardware required for accessible door passage shall be mounted no higher than 48 in (1220 mm) above finished floor. xv
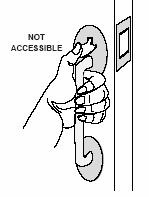
Figure 14 and 15 (top and bottom left) Non-accessible door handles
-
A thumb latch is not accessible because one must grasp the handle and pinch down on the thumb latch at the same time.
-
A round door knob (which requires tight grasping and twisting to operate) or a handle with a thumb latch are also inaccessible and should be modified or replaced, if doing so is readily achievable.

Accessible door handles

-
Figure 16: (left) A loop-type handle is accessible because it can be used without grasping, pinching or twisting.
-
Figure 17 (below) A lever handle is also accessible because it can be operated without a tight grasp, pinching or twisting.
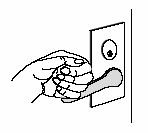

Tip: Close-fist test, try opening the door or operating the control using only one hand, held in a fist; if you can, than the door is usable by a broad range of people. The same is true for faucets, handles, drawer pulls, and vending machine controls.
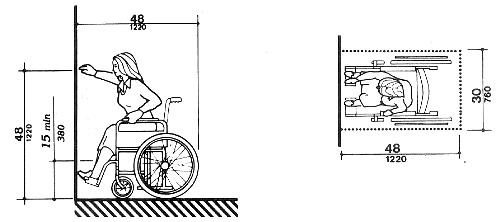
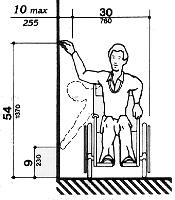
2. c. REACH RANGES
The maximum reach ranges (detailed below) should be considered in the placement of information brochures, magazines and other items located in medical office lobbies, reception, and waiting room areas. Figure 18 (high forward reach range), and Figure 19 (side reach range) illustrate reach ranges accessible to wheelchair users or people with limited mobility.
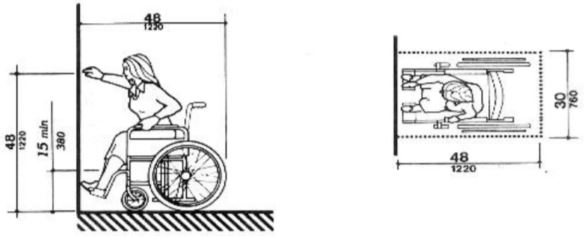
Figure 18: High forward reach limit: Forward reach range is 48 inches maximum and 15 inches minimum. xvi
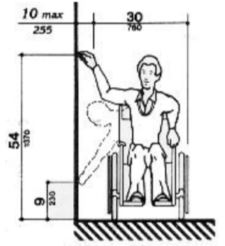
Figure 19: Side reach limits: The 30by48inch wheelchair clear floor space is located a maximum 10 inches (255 mm) from the wall. Side reach height range is 54 inches maximum and 9 inches minimum. xvii
2. c. i. Forward reach
Figure 18: High forward reach limit: Forward reach range is 48 inches maximum and 15 inches minimum.xvi
2. c. ii. Side reach
Figure 19: Side reach limits: The 30-by-48-inch wheelchair clear floor space is located a maximum 10 inches (255 mm) from the wall. Side reach height range is 54 inches maximum and 9 inches minimum.xvii
2. d. PATIENT RECEPTION DESKS
Reception desks should have a lower section where scooter and wheelchair users and people of short stature can easily communicate with staff. Compliant height range is 28 - 34 inches.xviii
Figure 20: Accessible reception desk Figure 21: Non-accessible reception desk


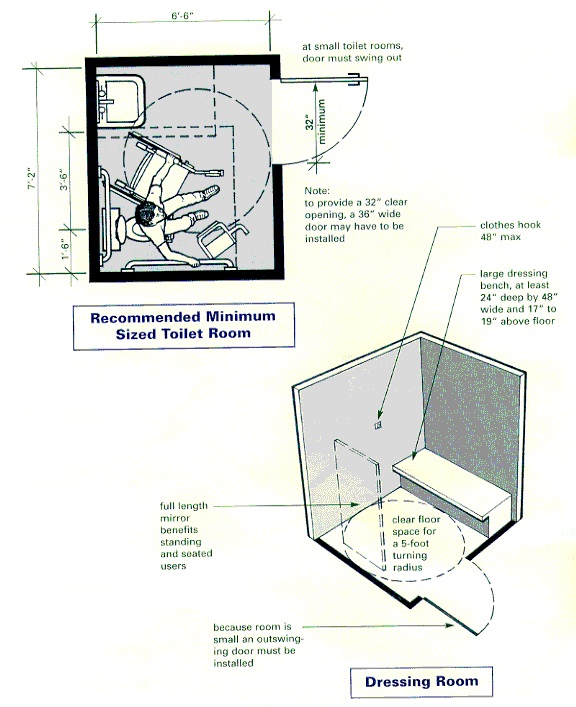
2. e. ACCESSIBLE TOILET AND DRESSING ROOMS
Figure 22: Diagram of features of an accessible dressing and toilet room.xix
3. FIXTURES and HARDWARE
Other fixtures and hardware can also prevent and/or limit access within medical exam and treatment rooms such as:
-
Accessible coat hooks,
-
Shelves,
-
Sinks and faucets, and
-
Restroom mirrors.
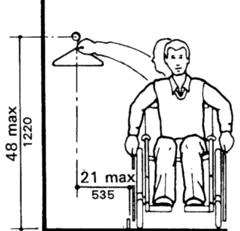
Coat hooks: “Accessible coat hooks provided within toilet compartments shall be located within the reach ranges specified above. When provided, a fold-down shelf shall be located 40 inches (1015 mm) minimum and 48 inches (1220 mm) maximum above the floor.”xx
Figure 23: Wheelchair side reach for coat hooks is 48 inches maximum above the floor, and 21 inches minimum. Forward reach range is 48 inches maximum and 21 inches minimum. (Diagram Figure 18 - page 10)
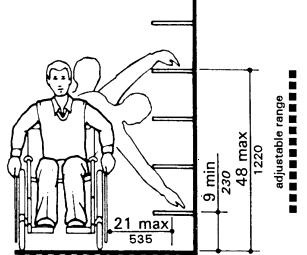
Shelves: “If the clear floor space allows a parallel approach by a person in a wheelchair and the distance between the wheelchair and the shelf exceeds 10 inches, the maximum high side reach shall be maximum 48 inches (1220 mm) above the floor and the low side reach shall be a minimum of 9 inches (230 mm) above the floor. Maximum distance from the user to the shelf shall be 21 inches (535 mm).”xxi
Figure 24: Wheelchair side reach range for wall shelving is 48 inches maximum above the floor. Forward reach range is 48 inches maximum and 15 inches minimum (Diagram Figure 19 page 11)
Lavatories:
-
Faucets: Must be “lever-operated, push-type, or electronically controlled mechanisms are examples of acceptable designs. If self-closing valves are used, the faucet shall remain open for at least 10 seconds.”xxii
Sinks
-
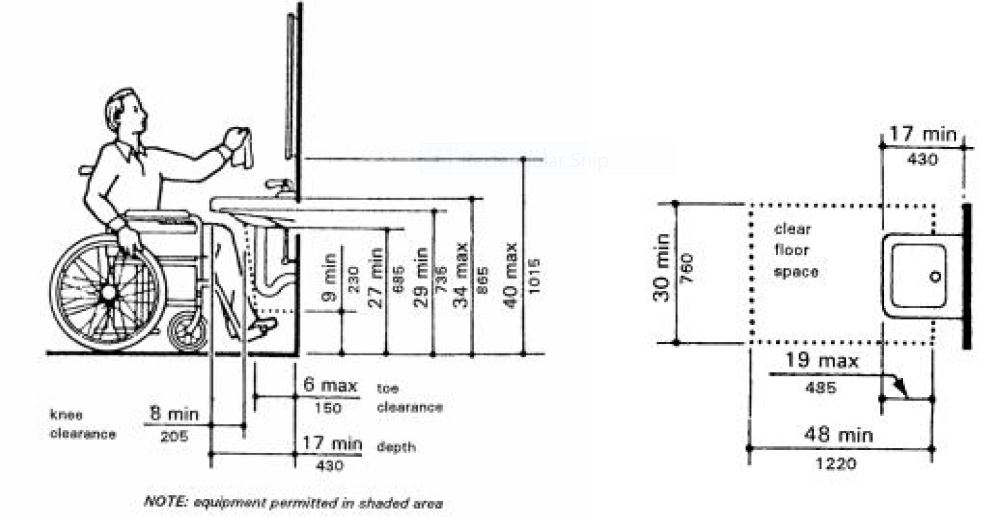
Exposed Pipes and Surfaces: Hot water and drain pipes under lavatories must be insulated or otherwise configured to protect against human contact. There shall be no sharp or abrasive surfaces under lavatories.
Figure 25: Wheelchair front approach lavatory knee clearance is required underneath the lavatory: 27 inches (685 mm) minimum from the floor to the underside of the lavatory which extends 8 inches (205 mm) minimum measured from the front edge underneath the lavatory back towards the wall.
Mirrors:xxiii
Figure: 26 Accessible lavatory mirror

Figure 27: Mirrors used by both ambulatory people and wheelchair users must be at least 74 in (1880 mm) high at their topmost edge.

4. a. ACCESS GUIDANCE DOCUMENTS
-
Checklist for Readily Achievable Barrier Removal
Easy-to-use survey tool for identifying barriers in facilities. The complete checklists and worksheets are the kind of documentation that organizations should keep on file to demonstrate that they are making a good faith effort to comply with the requirements of the ADA.
www.usdoj.gov/crt/ada/checkweb.htm -
Kailes, J., Americans with Disabilities Act Compliance Guide for Organizations,1995, (Hardcover)
Informal presentation on ADA compliance with chapters on: program access and nondiscrimination; physical access; communication access; and employment practices. Gives steps for completing an ADA compliance plan, contains checklists, planning sheets, samples of ADA compliance plans and lists many resources available for additional information and assistance. (Compliance with the transportation provisions of ADA is not covered).
www.jik.com/adacg.html
Email: jik@pacbell.net, www.jik.com -
Removing Barriers to Health Care: A Guide for Health Professionals, 1998.
This booklet provides guidelines and recommendations to help health care
professionals ensure equal use of the facility and services by all their patients. This
guide gives health care providers a better understanding of how to improve both the
physical environment and personal interactions with patients with disabilities
http://fpg.unc.edu/node/6264
PDF (335KB): http://fpg.unc.edu/node/6264
4. b. GOVERNMENT ADA PUBLICATIONS AND INFORMATION
-
-
U.S. Small Business Administration Office of Entrepreneurial Development,
U.S. Department of Justice Civil Rights Division
Americans with Disabilities Act (ADA) Guide for Small Businesses, October 15, 2002
www.sbaonline.sba.gov/ada/smbusgd.html
PDF (835 KB) www.sbaonline.sba.gov/ada/smbusgd.pdf
This 15-page illustrated guide presents an overview of basic ADA requirements for small businesses that provide goods and services to the public. It provides guidance on how to make their services accessible and how tax credits and deductions may be used to offset specific costs. -
Ten Small Business Mistakes (video)
This thirteen-minute video identifies common mistakes that small businesses make when trying to comply with the ADA and addresses the importance and value of doing business with 50 million people with disabilities. www.ada.gov/videogallery.htm#anchor10mistakes990
Available modes:-
Dial Up (Modem & ISDN) and High Speed Internet (DSL/Cable)
-
Quick Time | RealPlayer
-
Open Captions | Audio Description
-
-
-
ACCESSIBLE PARKING
The following two documents provide helpful information and diagrams on new construction requirements and restriping for accessible parking lot space requirements.-
Van-Accessible Parking Spaces
Technical Bulletin Parking
www.access-board.gov/Adaag/about/bulletins/parking.htm -
ADA Business Brief: Restriping Parking Lots (October 2001)
Department of Justice (DOJ)
www.ada.gov/restribr.htm
PDF (192 KB) www.ada.gov/restribr.pdf
-
-
THE ACCESS BOARD
1331 F Street, NW, Suite 1000
Washington, DC 200041111
Phone: 202.272.5434 (Voice) 202.272.5449 (TTY) 202.272.5447 (Fax)
Email: info@access-board.gov, https://www.access-board.gov/
The following Access Board sites provide information about the Americans with
Disabilities Act Accessibility Guidelines (ADAAG):-
ADAAG (Americans with Disabilities Act Accessibility Guidelines)
www.accessboard.gov/adaaba -
ADAAG Facility Access Surveys
www.accessboard.gov/adaag/checklist/a16.html -
ADAAG Technical Assistance
Email: ta@access-board.gov
Phone: (800) 8722253 (v)
(800) 9932822 (TTY)
Fax: (202) 2720081
-
-
ADA Information Line (DOJ)
800.514.0301 Voice/800.514.0383 TTY www.usdoj.gov/crt/ada/infoline.htm
Toll-free ADA Information Line provides information and free publications about the requirements of the ADA including the ADA Standards for Accessible Design.
Title II (State and Local Governments)
Title III (Public Accommodations)
Public Access Section, Civil Rights Division, U.S. Department of Justice
P.O. Box 66738 Washington, DC 200359998
1 (800) 5140301;1 (800) 5140383 TTY -
Disability and Business Technical Assistance Centers (DBTACs)
Phone: 800.949.4232 (V/TTY) https://adata.org/find-your-region
Regional centers to providing information, training, and technical assistance to employers, people with disabilities, and other entities under the ADA.
4. c. CUSTOMER SERVICE and COMMUNICATION and ACCESS
-
Reaching Out to Customers with Disabilities An online ADA course for businesses www.ada.gov/reachingout/intro1.htm
A 10-lesson course divided it into individual lesson modules. Modules allow you and your staff to learn at their own pace. Topics include:-
Policies & Procedures
-
Customer Communications
-
Accessible Design
-
Removing Barriers
-
Alternative Access
-
Maintaining Accessibility
-
Transporting Customer
-
Cost Issues
-
ADA Enforcement
-
Information Sources
-
-
Kailes, J., Language is More Than a Trivial Concern! November 1990, Revised 1999.
Sensitizes people to appropriate terminology to use when speaking with, writing about or referring to people with disabilities. Challenges readers to be aware of the importance of using disability-neutral
terms. Details preferred language and gives reasons for the disability community's preferences. Serves as an excellent reference tool for the public, media, marketers, providers and for board members, staff and volunteers of disability-related organizations. Includes a language quiz and many examples.
www.jik.com -
Kailes, J., Preferred Practices to Keep in Mind as You Encounter People Who Have Disabilities, Revised October 2000.
Describes practical approaches to use when serving or waiting on customers with physical, visual, hearing, cognitive, intellectual, and psychiatric disabilities, as well as people with significant allergies, asthma, multiple chemical sensitivities, and respiratory-related disabilities. Excellent training tool for people working with the public, includes a quiz as well as language and communication tips.
www.jik.com/gpam.html
Email: jik@pacbell.net -
Removing Barriers: Tips and Strategies to Promote Accessible Communication.
North Carolina Office on Disability and Health with Woodward Communications, 1999. Revised 2002. http://fpg.unc.edu/node/6265
PDF (1.24KB) 46 pages. http://fpg.unc.edu/sites/fpg.unc.edu/files/resources/other-resources/NCODH_PromoteAccessibleCommunication.pdf
Contains information on TTYs, etiquette for interacting with people with disabilities, web page design, audiovisual presentations, and print materials. Each topic is touched upon in enough depth to get you started on making communications more accessible.
ENDNOTES
i Title II applies to all public entities, defined as “any state or local government. 42 U.S.C. §12131 (2002). Section 504 applies to any entity that receives federal funding. 29 U.S.C. § 794. Federal financial assistance can be direct or indirect. Jacobson v. Delta Airlines, Inc., 742 F.2d 1202, 1211 (9th Cir. 1984).
ii Ibid.
iii Ibid.
iv The Access Board, ADAAG Standards, www.accessboard.gov/adaag
v Handinet, www.handinet.org/adaag.htm#4.3 (Accessible Route) The Access Board, ADAAG Standards.
vi The Access Board, ADAAG Standards, www.accessboard.gov/adaag/#4.6 4.6 Parking and Passenger Loading Zones
vii Mace, FAIA, Ronald L.,(1998), Center for Universal Design and The North Carolina Office on Disability and Health, Removing Barriers to Health Care: A Guide for Health Professionals.
viii The Access Board, ADAAG Standards, www.accessboard.gov/adaag/html/adaag.htm#A4.30.1 (Signage)
ix Ibid.
x Eye Catch Signs Limited, www.eyecatchsigns.com
xii The Access Board, ADAAG Standards
xiii Ibid.
xiv Ibid.
xv Ibid.
xvi Ibid.
xvii Ibid.
xviii Ibid.
xxi The Access Board, ADAAG Standards
xx Ibid.
xxi Ibid.
xxii Ibid.
xxiii Ibid.
User Comments/Questions
Add Comment/Question