The Impact of Transfer Setup on the Performance of Independent Transfers: Phase I Final Report
EXPERT REVIEW ON THE CURRENT KNOWLEDGE IN TRANSFERS
Chapter 1: Background
In 2002, the Access Board published the Accessibility Guidelines for newly construct or altered recreation facilities (1). These facilities include amusement rides, boating facilities, golf courses, and swimming pools among others. These guidelines establish minimum accessibility requirements to provide a general level of usability for people with disabilities. The recreation facility guidelines were developed with significant public participation including an advisory committee composed from representatives from different groups and organizations such as Paralyzed Veterans Association, Disabled American Veterans, International Association of Amusement Parks and Attractions, and Walt Disney Imagineering among others. The public was given an opportunity to comment on the proposed guidelines and the Board made changes based on this input. These recommendations were based on input from ride designers, persons with disabilities, along with established criteria for elements designed for transfer. Current standards have criteria only related to seat height and clear floor space for wheelchair users (2). The Access Board is interested in gathering additional data on transfers to develop guidelines (e.g. design criteria) for the purposes of enhancing accessibility for persons with mobility impairments. The primary goal of this project is to determine acceptable ranges for non-level transfers (e.g. vertical height differences), gaps between the transfer surface and wheelchair, and the clear space (length/width) needed to position the wheelchair in proximity to the target. Independent transfer was operationally defined as a transfer by which the individual requires no human assistance to perform. Setup was broadly defined as environmental type factors that impact transfer performance such as height and gap differences, space available next to the target element, and obstacles near or around transfer surfaces.
The first part of this study is a literature review that sought expert opinion on the relevance and strength of the evidence concerning set up and transfer performance. We sought to identify evidence in the literature that would provide insight into the burden that setup has to the performance of independent transfers Our goal was to evaluate the specific relevance related to transfer setup (i.e. vertical transfer distance; transferring across gap; number of transfers to go from the initial location to final surface; use of transfer assistive device). Results from the study will be used to identify where additional research is necessary to help define optimal design characteristics for transfer surfaces that have the least negative impact for wheeled mobility devices users who lived in community.
The second part is a study that was performed on 120 wheeled mobility device users who lived in the community to collect data on wheelchair transfers in order to make recreational facilities more accessible for people with mobility impairments. The aims included to study environmental variables such as vertical heights (e.g. transferring up/down), gaps between the target and wheelchair, clear space needed to position the wheelchair, and describe how transfer ability was affected by placing an obstacle (i.e. non-removable armrest) between the mobility device and the destination surface, and by providing a grab bar in front of the destination surface.
In this report, chapter 2 describes the methodology used for the literature review and data collection on transfers. Chapter 3 presents the results on the literature review and on the data collected on transfers. Finally, chapter 4 describes the implications of our results on current accessibility guidelines.
Objectives:
-
Research the literature for evidence on the impact of setup on independent transfers
-
Collect data on different setups
-
Compare results to current accessibility guidelines for amusement rides in terms of minimum clear floor areas, height, obstacle, and grab bar use.
1. Accessibility Guidelines for Recreation Facilities, (2002).
2. Accessible amusement rides - a summary of accessibility guidelines for recreation facilities. US Access Board; 2003.
Expert opinion on the current literature
Scientific literature databases were searched until June 2009 using 43 keywords resulting in 339 articles. These were internally reviewed and narrowed to 41 articles which were formally assessed by thirteen external experts. Articles that 80% or more of the reviewers scored as moderately or highly relevant were included in the results. Titles and abstracts of the articles were reviewed internally by two experts with at least four years of direct clinical and research experience working with full-time wheelchair users. Articles that both experts agreed were relevant to the performance of independent wheelchair transfers were selected for the next step of review. Thirteen external reviewers who are collaborators and work in the assistive technology and/or the rehabilitation field were invited to participate in a study to formally evaluate the remaining studies. Two reviewers held at minimum a bachelor’s degree, seven reviewers master’s degree, one was a physician and three held PhD degrees. All the reviewers had greater than five years of clinical research and/or practical clinical experience. The study was approved by the University of Pittsburgh Institutional Review Board.
External reviewers were sent a cover letter that described the purpose of the study and asked them to score each of the articles identified by the internal reviewers using a scoring sheet specifically devised for this study (Appendix 1).
Subjects
The target sample required wheeled mobility device users who lived in the community and were able to transfer independently (with or without a transfer board) and who represent a broad spectrum of disabilities. Subjects were eligible to participate if they (1) were at least 18 years old, (2) able to independently perform a transfer to/from a WMD with or without transfer board, (3) owned a WMD, and (4) had been using the WMD for at least one year. Subjects were excluded from the study if they had (1) significant upper extremity pain or injury that would inhibit the ability to perform transfers (2) active or recent history of pressure sores pressure sores.
Subjects were tested at the 24th National Disabled Veterans Winter Sport Clinic in Snowmass Village, Colorado during March 2010; at the 30th National Veterans Wheelchair Games in Denver, Colorado during July 2010; at the Hiram G Andrews Center in Johnstown, Pennsylvania during November 2010 and March 2011; during the US Access Board Meeting in Chicago, Illinois during September 2010; at the Human Engineering Research Laboratories in Pittsburgh, Pennsylvania between June 2010 and April 2011; and at H. John Heinz III VA Progressive care center in June 2011.
Measures and Procedures
A custom-built modular, transfer station was designed and built and consisted of a height adjustable platform capable of a range between 10” to 29” with increments every inch (25.4-73.7 cm in 2.5 cm) with a fixed backrest 17” wide by 25” high (63.5x43.2 cm) and a 95° recline; a lateral grab bar (fixed height of 32” or 81.3 cm) and allows for attaching/detaching side guards (e.g. obstacle to transfer) and an optional front grab bar of varying height (Figure 1) of 19”-38” (48.3-96.5 cm) with increments every 2” (5.1 cm). The grab bars’ diameter is 1.5” (3.8cm). The space for the legs and feet has a fixed dimension of 14.5” deep by 22.5” wide (36.8x57.2cm).
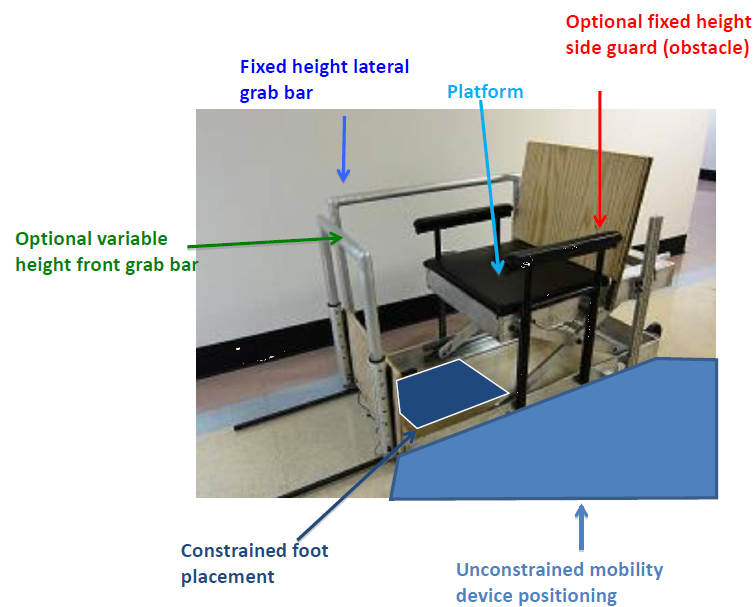
Figure 1 . Custom-built transfer station with the front grab bar, lateral grab bar, side guard, feet space, and space for WMD positioning highlighted.
For the initial setup, the platform was adjusted to be level with the subject’s WMD seat, with no side guard or front grab bar in place. The subjects were asked to position themselves next to the platform as they normally would to prepare for a transfer. Angular orientation and linear distances of the WMD with respect to the front most corner of the platform were recorded (Figure 2). Each subject was asked to perform a transfer from their WMD to the station and back to their WMD. Grab bar(s) use was noted. Next, they were asked to perform five protocols in random order. Subjects were asked to exercise sound judgment in performing the transfers and to only do transfers they felt comfortable and safe doing. Subjects were spotted in the event they would begin to slip/fall during a transfer in which the case the transfer was declared ‘unattainable’. After each transfer in each protocol, changes made to device positioning (x, y, α, Figure 2) and leading/trailing hand placement were recorded. The angle between the WMD and the transfer station is defined from 0°-180°. When the WMD is parallel to the transfer station and the subject is facing towards the front of the station the angle is defined as 0° and when the WMD is parallel to the transfer station but the subject is facing towards the back of the station the angle is defined as 180°.
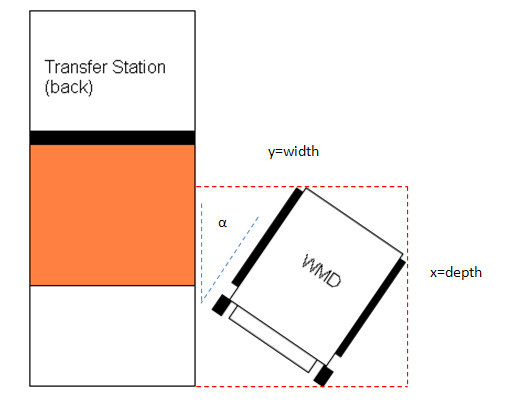
Figure 2 . WMD position measures taken to calculate the overall space needed to transfer
Adjustable height protocol: From initial setup, only the height of the platform was adjusted incrementally: higher (Figure 3) and lower than the subject’s seat. The amount of vertical distance that the seat was raised/lowered each time depended on the subject’s perceived and observed transfer abilities. The maximum and minimum heights the subject could transfer to/from the platform were recorded. As WMD seat heights differed among subjects, we also computed the difference between their seat height and the absolute maximum and minimum height they attained to calculate height differentials.

Figure 3 . Subject transferring to the transfer station set at a higher (left) and lower (right) height than the wheelchair
Adjustable gap protocol: From initial setup, just the horizontal distance between the WMD and platform was incrementally increased by placing plywood blocks of 3.5” (8.9cm) width between the transfer station and the WMD (Figure 4). The platform height remained level with their WMD seat height. The amount of horizontal distance increased each time again depended on the subjects perceived and observed transfer abilities. The maximum horizontal distance the subject could transfer to/from the platform was recorded.

Figure 4 . Person transferring with a 7in gap and the transfer station height at level with the wheelchair
Adjustable height/gap protocol: From the initial setup, a gap separating the device and platform was introduced with the plywood blocks of 3.5” (8.9cm) and then the height of platform was adjusted incrementally higher/lower (Figure 5). This procedure was repeated until the largest horizontal distance was reached. The maximum and minimum heights attainable with the largest horizontal distance were recorded.

Figure 5 . Subject transferring with a 7in gap and the transfer station higher than the wheelchair.
Side guard protocol: From initial setup, two side guards adjusted 6” (15.2 cm) higher than the subject’s WMD seat were attached, and subjects were asked to perform a level height transfer. Then the height of the platform was adjusted incrementally in height: higher and lower than the subject’s seat and the maximum transfer heights high/low that were attainable were recorded (Figure 6). Then from initial setup, the horizontal distance between the wheelchair and platform was incrementally increased and the maximum attainable gap distance was recorded. For all transfers with the side guard, side guard height was adjusted to be 6” higher than the WMD seat when the platform was level or lowered and 6” above the platform height when the platform was raised.

Figure 6 . Subject transferring with the side guard in place and the transfer station higher than the wheelchair
Front grab bar protocol: From the initial setup, an adjustable height grab bar was placed in front of the platform which enabled an additional optional handheld to assist with transferring to/from the platform. The horizontal distance between the center of the grab bar and the mid-center, front edge of the platform was 13.5”. Two conditions in random order were tested: 1) front grab bar and no side guard and 2) both front grab bar and side guard present in the setup. Subjects first performed a level height transfer in each condition and afterwards performed the variable height portion of the protocol as described previously (e.g. Adjustable height protocol). For each condition (e.g. grab bar with side guard and grab bar without side guard), subjects were asked to select their preferred grab bar height for both 1) transferring to lower heights and 2) transferring to higher heights than their WMD seat height. The preferred grab bar height was measured between the floor and the top of the grab bar surface. Maximum and minimum heights attainable, front grab use, and grab bar heights for each the lower-height and higher-height transfers were recorded.

Figure 7. Subject transferring with the side guard and front grab bar in place and the transfer station higher than the wheelchair
Data analysis
The number of subjects that attempted to perform each protocol and the number of subjects that were not able to attain the transfer(s) with that configuration are reported for each protocol. Descriptive statistics (e.g. means, medians, frequencies, standard deviations) of the data were calculated for the subjects that were able to attain the transfers in each protocol. Population proportion confidence intervals (CI) were determined at 95%. We compared our results with the current accessibility standards.
Expert opinion on current literature
Nineteen articles met the relevancy criteria. The aspects of setup that experts felt were addressed to some degree included vertical transfer distance, transferring across a gap and position of the mobility device relative to target destination.
None of the 19 articles were scored as having strong to very strong resulting evidence. There is a consensus among studies that transferring to a higher surface implies greater exertion of the upper limb (3-6) . However, there were no studies that specifically investigated the range of heights feasibly attainable by subjects which is important for determining the suitability of existing accessibility guidelines concerning transfers (7). There was not enough evidence in any one study or combination thereof that would enable for determining how high or low, how close, and how much space is needed next to the target surface so it can be accessible by a majority of wheelchair users.
3. Nyland J, Quigley P, Huang C, Lloyed J, Harrow J, Nelson A. Preserving transfer independence among individuals with spinal cord injury. Spinal Cord. 2000;38(11):649-57.
4. Gagnon D, Nadeau S, Noreau L, Eng J, Gravel D. Trunk and upper extremity kinematics during pivot transfers performed by individuals with sipanl cord injury. Clinical Biomechanics (Bristol, Avon). 2008;23(3):279-90.
5. Gagnon D, Nadeau S, Noreau L, Eng J, Gravel D. Electromyographic patterns of upper extremity muscles during sitting pivot transfers performed by individuals with spinal cord injury. Journal of Electromyography and Kinesiology. 2009;19(3):509-20.
6. Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, McFadyen B. Movement patterns and muscular demands during posterior transfers toward an elevated surface in individuals with spinal cord injury. Spinal Cord. 2005;43(2):74-84.
7. Americans with Disabilities Act and Architectural Barriers Act Accessibility Guidelines. In: Board USA, editor. Washington DC 2004.
Subjects
The sample consisted of 95 men and 25 women with an average age of 47.7 ± 15.3 years, body weight of 77.8 ± 21.8 kg, and height of 1.70 ± 0.14 m. We enrolled subjects with a broad variety of disabilities ranging from spinal cord injury (SCI), multiple sclerosis (MS), cerebral palsy (CP), and post-polio among others.
Table 1 contains the self-reported type of disabilities and the number of subjects that reported them. We asked those with spinal cord injury to report their level of injury as well as type of injury (complete or incomplete). Table 2 contains the self-reported levels of spinal cord injuries (C-cervical, T-Thoracic, and L-Lumbar) for the subjects that reported only spinal cord injury as their type of disability; 59% of this group reported having incomplete spinal cord injuries.
Table 1 . Subjects’ self-reported type of disability (n=120).
| Disability |
Number of subjects |
|
Spinal cord injury |
54 |
|
Multiple sclerosis |
10 |
|
Cerebral palsy |
11 |
|
Lower extremity amputation |
9 |
|
Spina bifida |
6 |
|
Multiple sclerosis and spinal cord injury |
3 |
|
Osteogenesis imperfect |
2 |
|
Post-polio |
2 |
|
Traumatic brain injury and spinal cord injury |
2 |
|
Traumatic brain injury and lower extremity amputation |
1 |
|
Muscular dystrophy |
2 |
|
Rheumatoid arthritis |
2 |
|
Traumatic brain injury |
2 |
|
Spinal cord injury and lower extremity amputation |
1 |
|
Osteoporosis |
1 |
|
Stroke |
1 |
|
Adams-Oliver syndrome |
1 |
|
Ambulatory Dysfunction |
1 |
|
Reflex sympathetic dystrophy |
1 |
|
Spinal stenosis |
1 |
|
Epidemiral cyst |
1 |
|
Double lower extremity amputation and stroke |
1 |
|
Amyotrophic lateral sclerosis |
1 |
|
Respiratory problems |
1 |
|
Sarcoidosis |
1 |
|
Knee replacement complications |
1 |
|
Hip injury |
1 |
Table 1 Alternative Text Description: This table gives the Subjects’ self-reported type of disability. There are two columns; the left side lists the disability and the right side gives the number of subjects who reported having that disability. The total number of subjects adds up to 120.
Table 2 . Level of spinal cord injury for the subjects that only self-reported SCI as their disability (n=54).
| Level of injury |
Number of subjects |
|
C3 |
1 |
|
C4 |
2 |
|
C5 |
2 |
|
C6 |
4 |
|
C7 |
2 |
|
T2 |
1 |
|
T3 |
2 |
|
T4 |
2 |
|
T5 |
4 |
|
T6 |
3 |
|
T7 |
6 |
|
T8 |
2 |
|
T9 |
2 |
|
T10 |
1 |
|
T11 |
6 |
|
T12 |
5 |
|
L1 |
2 |
|
L2 |
1 |
|
L4 |
3 |
|
Not reported |
3 |
Abbreviation: C= Cervical, T=Thoracic, L=Lumbar
Table 2 Alternative Text Description: This table gives the level of spinal cord injury for the subjects that only self-reported SCI as their disability. There are two columns; the left side list the level of injury and the right side lists the number of subjects who reported having that level of spinal cord injury. The total number of subjects that reported SCI as their disability was 54.
The sample as a whole had been using a WMD for 14.9 ±12.1 years with a range from 1 to 59 years. Wheelchair seat plus the cushion height measured at the edge was 21.6 ± 1.4” (54.8 ± 3.4 cm) median was 22” (55.8 cm) and range: 17 – 25” (43.2 – 63.5 cm). There were 84 manual wheelchair, 29 power wheelchair, 5 scooter, and 2 power assist users. 18% (22/120) reported using assistive technology for transfers: 14 used transfer board, 3 lifts, 3 canes, and 2 walkers.
Four of the 120 subjects enrolled in the study met inclusion criteria for independent transfer but were unable to transfer to/from the station based on space constraints and their method of approach. All these subjects were power wheelchair users except for subject S4 who used a manual wheelchair. Subject S3 used a transfer board in his transfers. This group’s demographics are expanded in The remaining 116 subjects completed all or portions of the study. The reason for not completing all portions of the study was mainly due to time constraints, such as having to end participation in the study because the participants were short on time. Figure 8 summarizes the number of subjects for each protocol. A few subjects ended the study early due to experiencing fatigue or pain. The average number of transfers performed during the study was 22.9 ± 9.6 (range: 0-48). Moving from the WMD to the transfer station and from the transfer station to the WMD counted as two transfers.
Table 3. Demographics characteristics of the subjects who were not able to attain any transfers.
Subject ID |
Diagnosis |
Gender |
Age |
Weight |
Height |
Years using WMD |
|
S1 |
Cerebral palsy |
Male |
57 |
140lbs (63.5kg) |
68in (1.73m) |
52 |
|
S2 |
Cerebral palsy |
Male |
Unknown |
Unknown |
Unknown |
Unknown |
|
S3 |
Stroke and double above knee amputee |
Male |
55 |
250lbs(113.4kg) |
72in (1.83m) |
4 |
|
S4 |
Cerebral palsy |
Female |
41 |
160lbs(72.6kg) |
57in (1.45m) |
40 |
Table 3 Alternative Text Description: This table gives the demographic characteristics of the subjects who were not able to attain any transfers. The table lists four subjects (three male and one female). Three of the subjects had cerebral palsy and one had a stroke and double above knee amputation. The numbers of known years each of these subjects have been using a WMD ranges from 4-52 years.
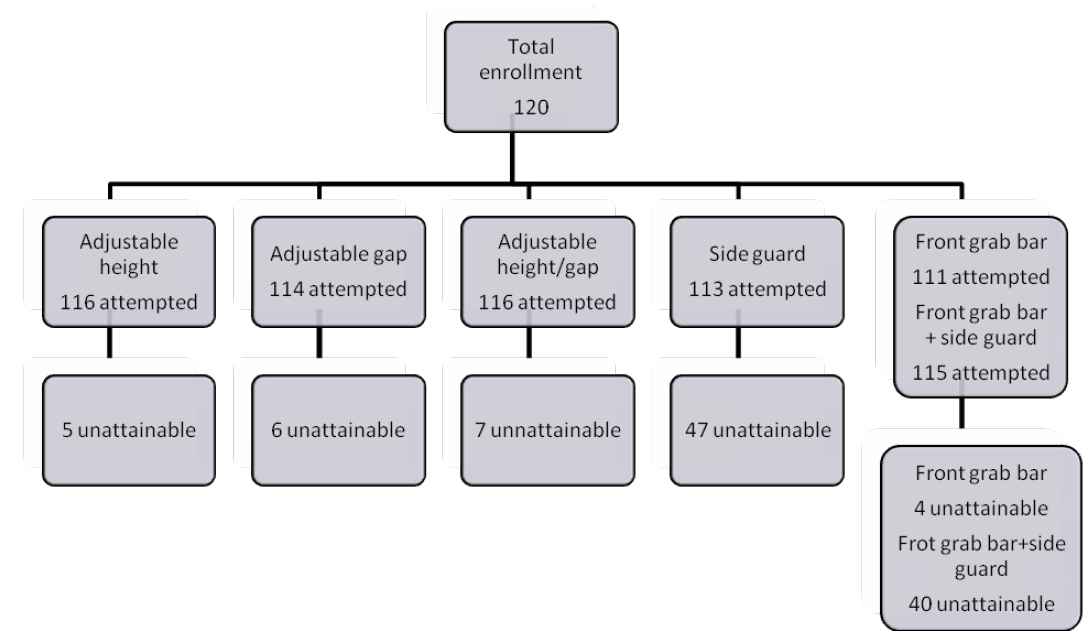
Figure 8 . Total number of subjects that attempted each protocol and that were unattainable.
Adjustable height protocol
One hundred and sixteen (116) subjects were tested under this protocol and five were unable to transfer to the platform at any height in the configuration shown in (Figure 3). 92%, CI[86%,96%] of the sample (107/116) could transfer at a height of 22” (50.8cm). Fewer numbers of subjects could transfer above and below this height (Figure 9 and Table 4).
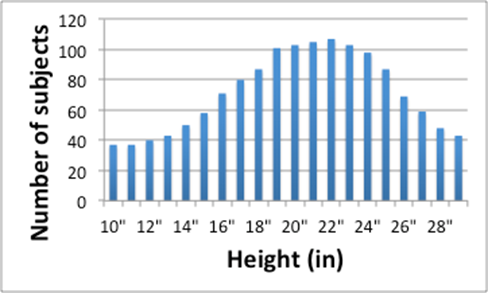
Figure 9 . Number of subjects (y-axis) able to transfer at each height increment (x-axis).
Table 4 . Percentage of subjects that were able to attain a transfer under adjustable height protocol
| Height (in) |
% Subjects Adjustable Height |
% Subjects Side guard |
|
10 |
28% |
24% |
|
11 |
28% |
25% |
|
12 |
34% |
26% |
|
13 |
37% |
27% |
|
14 |
43% |
27% |
|
15 |
49% |
31% |
|
16 |
62% |
35% |
|
17 |
69% |
40% |
|
18 |
75% |
41% |
|
19 |
88% |
43% |
|
20 |
89% |
48% |
|
21 |
91% |
51% |
|
22 |
92% |
52% |
|
23 |
90% |
51% |
|
24 |
85% |
46% |
|
25 |
73% |
46% |
|
26 |
60% |
41% |
|
27 |
50% |
38% |
|
28 |
42% |
27% |
|
29 |
37% |
22% |
Table 4 Alternative Text Description: This table gives the percentage of subjects that were able to attain a transfer under the adjustable height protocol compared to the percentage of subjects that were able to attain the transfer with the side guard in place. There are three columns; the left one lists the transfer height in inches, the middle one lists the percentage of subjects that attained the adjustable height transfer, the right one lists the percentage of subjects that attained the adjustable height transfer with the side guard.
Table 5 contains the height differentials that subjects were able to attain. For each participant, these height differentials were calculated as the relative height difference by subtracting the maximum attainable height (high and low) to the WMD seat height. The results suggest that 2” transfer heights above and below the WMD seat height are acceptable for at least 86% of the subjects that could attain the Adjustable Height protocol.
Table 5 . Percentage of subjects that were able to attain step heights.
| Relative Heights (in) |
Attainable (%) |
|
-6 |
57% |
|
-5 |
64% |
|
-4 |
69% |
|
-3 |
78% |
|
-2 |
86% |
|
-1 |
96% |
|
0 |
96% |
|
1 |
94% |
|
2 |
89% |
|
3 |
76% |
|
4 |
63% |
|
5 |
51% |
|
6 |
43% |
Table 5 Alternative Text Description: This table gives the percentage of subjects that were able to attain step heights. There are two columns; the left one lists the relative heights attained in inches, the right one lists the percentages of subjects that were able to attain that height.
Subjects that could not attain the protocol
In addition to the 4 subjects that could not attain any of the protocols, two additional subjects (1 woman, 1 man) could not attain the adjustable height protocol. The woman was 51 years old and had a an incomplete spinal cord injury at level L4, weighted 170 lbs, was 64” tall, and had been using a manual wheelchair for one year. The man was 68 years old and had a complete spinal cord injury at level T2, weighted 185 lbs, was 71” tall, had been using a manual wheelchair for 7 years, and used a walker to aid with his transfers.
Subjects that could not attain the protocol
In addition to the 4 subjects that could not attain any of the protocols, two additional subjects (1 woman, 1 man) could not attain the adjustable height protocol. The woman was 51 years old and had a an incomplete spinal cord injury at level L4, weighted 170 lbs, was 64” tall, and had been using a manual wheelchair for one year. The man was 68 years old and had a complete spinal cord injury at level T2, weighted 185 lbs, was 71” tall, had been using a manual wheelchair for 7 years, and used a walker to aid with his transfers.
Adjustable gap protocol
One hundred and fourteen (114) subjects were tested under this protocol and six could not transfer with a gap of any size added between their WMD and the platform in the configuration shown in (Figure 4). 95% (108/114) of the sample were able to safely attain a level transfer with a gap of 3.5” (8.9 cm). Around 81% (92/114), CI[72%,87%] of the sample were able to transfer with a gap of 7” (17.8 cm) or less (Figure 10 and Table 6).
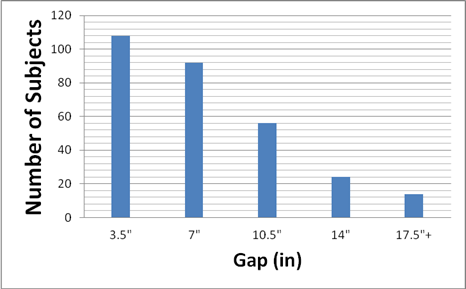
Figure 10 . Number of subjects (y-axis) able to transfer with a certain gap (x-axis).
Table 6 . Percentage of subjects that a transfer under adjustable gap protocol
| Gap |
% of subjects |
|
3.5" |
95% |
|
7" |
81% |
|
10.5" |
49% |
|
14" |
21% |
|
17.5"+ |
12% |
Table 6 Alternative Text Description: This table gives the percentages of subjects that attained a transfer under the adjustable gap protocol for different gap distances. There are two columns; the left one gives the gap distance range, the right one gives the percentage of subjects that were able attain that gap distance.
Subjects that could not attain the protocol
In addition to the 4 subjects that could not attain any of the protocols, two additional men could not attain the adjustable gap protocol. One was a 41 year old men that had a traumatic brain injury and double lower knee amputation, weighted 192 lbs, did not report his height, and had been using a manual wheelchair for twenty years. The second subject was 68 years old and had a complete spinal cord injury at level T2, weighted 185 lbs, was 71” tall, had been using a manual wheelchair for 7 years, and used a walker to aid with his transfers. This last subject could not attain the adjustable height protocol as mentioned above.
Adjustable height/gap protocol
One-hundred and sixteen (116) subjects were tested under this protocol, of which seven were unable to transfer with a height/gap combination in the configuration shown in (Figure 5). 86% (100/116), CI [79%, 91%] of the sample were able to attain a height of 22” (55.9 cm) with a gap of 3.5” ( 7.6 cm). The number of subjects who are able to achieve transfers for any height beyond a 7" (17.8 cm) gap distance dropped off dramatically (Figure 11 and Table 7).
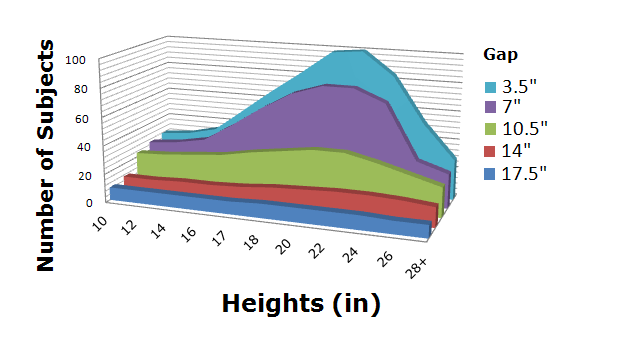
Figure 11 . Number of subjects (z-axis) able to attained a certain gap (y-axis) at a certain height (x-axis).
Table 7 . Number of subjects that were able to attain a certain gap at a certain height under adjustable height/gap protocol
| Height\Gap |
3.5" |
7" |
10.5" |
14" |
17.5"+ |
|
10" |
24% |
22% |
20% |
9% |
8% |
|
12" |
26% |
24% |
21% |
9% |
8% |
|
14" |
30% |
28% |
22% |
10% |
8% |
|
16" |
44% |
39% |
24% |
10% |
8% |
|
17" |
58% |
51% |
28% |
11% |
8% |
|
18" |
71% |
61% |
30% |
13% |
9% |
|
20" |
84% |
67% |
33% |
14% |
9% |
|
22" |
86% |
67% |
33% |
15% |
9% |
|
24" |
72% |
59% |
28% |
15% |
9% |
|
26" |
45% |
27% |
23% |
14% |
8% |
|
28"+ |
24% |
21% |
18% |
12% |
8% |
Table 7 Alternative Text Description: This table gives the number of subjects that were able to attain a certain gap at a certain height under the adjustable height/gap protocol. There are seven columns; the left one lists the height of the transfer in inches, the rest of the columns list the percentages of subjects that could attain the transfer at increasing gap distances. The number of subjects who were able to achieve transfers for any height beyond a 7” (17.9 cm) gap distance dropped off dramatically.
Subjects that could not attain the protocol
In addition to the 4 subjects that could not attain any of the protocols, three additional men could not attain the adjustable height/gap protocol. One had a complete spinal cord injury at level L4, weighted 145 lbs, 67” tall, and had been using a manual wheelchair for twenty years and used a transfer board during transfers. The second subject had a complete spinal cord injury at level T2, weighted 185 lbs, was 71” tall, had been using a manual wheelchair for 7 years, and used a walker to aid with his transfers. This subject could not attain the adjustable height protocol and adjustable gap as mentioned above. The last subject of this group was a 69 year old men who had amyotrophic lateral sclerosis, weighted 130 lbs, 67” tall, and had been using a power wheelchair for one year.
Side guard protocol
One-hundred and thirteen (113) subjects were tested under this protocol. As described above, side guard height was adjusted to be 6” higher than the WMD seat when the platform was level or lowered and 6” above the platform height when the platform was raised. 42% (47/113), CI[30%,47%] of the subjects could not achieve a transfer with the side guard in place and with the platform at level with the WMD. When the conditions were changed (height raised/lowered or gap introduced) the transfers were unattainable to up to 47% (53/113), CI[37%,55%] of the participants. Of the 60 subjects that were able to transfer to a higher level than their own WMD, 98% (59/60), CI[91%,99%] were able to transfer to height of 22” (55.9cm) (Figure 12 and Table 8). At the extreme ranges of platform heights 22% (25/113), CI[24%,31%] were able to transfer to the highest height of 29” (73.7 cm). 24% (27/113), CI[17%,32%] were able to transfer to the lowest height of 10” (25.4cm).
When a gap was introduced with the side guard 60 subjects were able to attain this transfer. 41% (46/113), CI[34%,52%] were able to transfer at a height level with their WMD and a gap of 7" (17.8 cm). Only6% (7/113), CI[4%,13%] could transfer with a 17.5” (40.6cm) or greater gap (Figure 13 and 9).
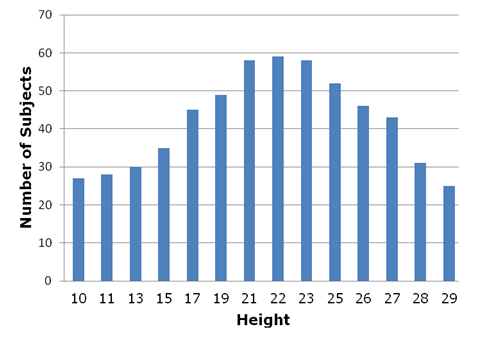
Figure 12. Number of subjects (y-axis) able to transfer at different heights (x-axis) with the side guard in place.
Table 8 . Percentage of subjects that were able to attain a certain height in the side guard protocol
|
Height (in) |
% Subjects Side guard |
|
10 |
24% |
|
11 |
25% |
|
12 |
26% |
|
13 |
27% |
|
14 |
27% |
|
15 |
31% |
|
16 |
35% |
|
17 |
40% |
|
18 |
41% |
|
19 |
43% |
|
20 |
48% |
|
21 |
51% |
|
22 |
52% |
|
23 |
51% |
|
24 |
46% |
|
25 |
46% |
|
26 |
41% |
|
27 |
38% |
|
28 |
27% |
|
29 |
22% |
Table 8 Alternative Text Description: This table gives the percentage of subjects that were able to attain a certain height during the side guard protocol. There are two columns; the left one lists the transfer height, the right one lists the percentage of subjects that were able to attain that height.
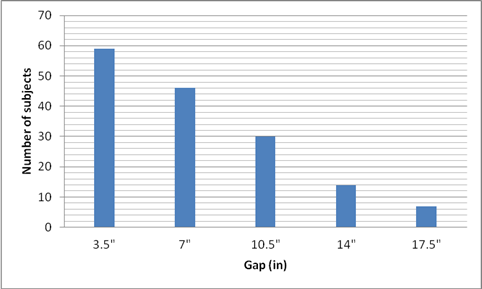
Figure 13. Number of subjects (y-axis) able to transfer with different gaps (x-axis) at a level transfer with the side guard in place
Table 9 . Percentage of subjects that were able to attain a certain gap in the side guard protocol
Gap |
% Subjects |
|
3.5" |
52% |
|
7" |
41% |
|
10.5" |
27% |
|
14" |
12% |
|
17.5" |
6% |
Table 9 Alternative Text Description: This table gives the percentage of subjects that were able to attain a transfer with a certain gap during the side guard protocol. There are two columns; the left one list the gap distances; the right one list the percentages of subjects that were able to attain the transfer at that gap distance. Forty-one percent of the subjects were able to transfer at a height level with their WMD and a gap of 7 inches. Only 6% could transfer with a 17.5 inch or greater gap.
Subjects that could not attain the protocol
In addition to the 4 subjects that could not attain any of the protocols, forty-three additional subjects could not attain the side guard protocol. Table 10 contains basic demographic characteristics of these 43 subjects.
Table 10 . Demographics of the subjects that could not attain protocol side guard.
| Diag-nosis |
Gender |
Age |
Weight (lbs) |
Height (lbs) |
Years using WMD |
Type of WMD |
AT for transfers |
|
SCI T7-C |
M |
40 |
142 |
67 |
15 |
M |
|
|
SCI T6-C |
M |
47 |
216 |
74 |
1 |
M |
|
|
SCI T11 –C |
M |
34 |
130 |
70 |
2 |
M |
|
|
MS |
M |
52 |
203 |
71 |
10 |
P |
Transfer board |
|
RSD |
F |
37 |
118 |
62 |
5 |
M |
Transfer board |
|
MS |
M |
62 |
180 |
60 |
37 |
S |
|
|
SCI |
M |
56 |
165 |
62 |
22 |
M |
|
|
SCI T5-I |
M |
57 |
160 |
72 |
16 |
M |
|
|
AK amputee |
M |
62 |
245 |
69 |
11 |
P |
|
|
SCI L1 –C |
M |
65 |
150 |
68 |
25 |
M |
|
|
SCI L3-I/LAKA |
M |
65 |
211 |
72 |
13 |
P |
|
|
SCI C5 –I |
M |
53 |
160 |
71 |
26 |
M |
Transfer board |
|
SCI L4 –I |
M |
71 |
228 |
70 |
10 |
P |
|
|
SCI T11-C |
M |
65 |
195 |
70 |
4 |
P |
Transfer board |
|
SCI T11- I |
M |
46 |
194 |
68 |
16 |
M |
|
|
MS |
M |
58 |
205 |
69 |
20 |
M |
Transfer board |
|
SCI T3 –I |
M |
55 |
225 |
56 |
10 |
M |
|
|
SCI T12 –C |
M |
61 |
150 |
70 |
4 |
M |
|
|
MS |
F |
61 |
125 |
69 |
N/A |
M |
|
|
CP |
M |
57 |
140 |
68 |
52 |
P |
|
|
SCI T12-I |
M |
54 |
190 |
72 |
30 |
M |
|
|
MS |
M |
36 |
160 |
63 |
9 |
M |
|
|
Post polio |
F |
66 |
250 |
62 |
56 |
M |
|
|
SCI C6 –I |
M |
29 |
120 |
70 |
5 |
M |
|
|
SCI T5 –I |
M |
31 |
170 |
73 |
10 |
S |
|
|
SCI L3 -I |
M |
39 |
287 |
69 |
15 |
M |
|
|
SCI T4- C |
M |
35 |
165 |
72 |
17 |
M |
|
|
CP |
F |
22 |
140 |
63 |
12 |
M |
|
|
Spina Bifida |
F |
20 |
110 |
60 |
20 |
M |
|
|
CP |
53 |
M |
190 |
72 |
24 |
P |
|
|
SCI T7 -C |
M |
63 |
115 |
63 |
24 |
M |
|
|
CP |
M |
46 |
158 |
69 |
16 |
S |
|
|
SCI T6-C |
M |
46 |
158 |
69 |
16 |
M |
|
|
Doble AKA-Stroke |
M |
55 |
250 |
72 |
4 |
P |
|
|
SCI T3-C |
M |
27 |
110 |
67 |
12 |
M |
|
|
SCI C7-I |
F |
48 |
170 |
65 |
3 |
M |
|
|
SCI L1- C |
F |
55 |
115 |
66 |
30 |
M |
|
|
SCI C6- I |
F |
33 |
180 |
77 |
5 |
M |
|
|
CP |
F |
41 |
160 |
57 |
40 |
M |
|
|
SCI T12-I |
M |
58 |
N/A |
74 |
28 |
M |
|
|
SCI C5 – I |
M |
49 |
161 |
70 |
25 |
M |
|
|
RA |
F |
44 |
230 |
64 |
18 |
M |
Transfer board |
|
SCI T7-C/TBI |
M |
29 |
200 |
70 |
6 |
M |
Transfer board |
|
TBI |
M |
43 |
180 |
70 |
28 |
P |
|
|
SCI T4-C |
M |
41 |
170 |
67 |
21 |
P |
Transfer board |
|
Spina Bifida |
F |
40 |
145 |
59 |
29 |
M |
|
|
SCI T11 -I |
F |
24 |
235 |
72 |
3 |
M |
Transfer board |
|
Total |
12 F |
47±13 |
175±42 |
68±5 |
18±12 |
34M |
10 used TB |
|
|
35 M |
3 S |
Abbreviation: SCI-spinal cord injury, C-complete, I-incompelte, MS- multiple sclerosis, RSD-reflex sympathetic dystrophy, CP-cerebral palsy, AK-above knee, RA- rheumatoid arthritis, N/A data not reported.
Table 10 Alternative Text Description: This table gives the demographics of the subjects that could not attain the side guard protocol. Forty-three subjects could not attain the side guard protocol.
Grab bar protocol
One hundred and fifteen (115) subjects were tested under this protocol and four were unable to perform any transfers because this particular configuration posed significant barriers to their transfer. These four subjects were the ones that could not attain any of the other protocols.
When transferring to a lower height, with the front grab bar available, and without side guard, 51% (59/115), CI[42%,60%] used the front bar, and 20% (23/111), CI[12%,25%] could transfer to a lower height when using the bar, and the bar height preference was 30 ± 3.9” (76.2±9.9cm) median 30” (76.2cm). When transferring to a higher height, with the front grab bar, and without side guard, 59% (68/115), CI[50%,68%] used the front bar, 17% (20/115), CI[12%,25%] could transfer to a higher height when using the bar, and the bar height preference was 33.4 ± 3.1” median 32” (84.8±7.8cm, median 81.3 cm).
One-hundred and fifteen subjects performed the part of the protocol that included the side guard. 65% (75/115), CI[56%,73%] attained the transfer at level with their WMD and 10% (11/115) , CI[5%,16%] of the subjects who could not transfer with the side guard in place in the previous protocol could transfer with the grab bar in front. When transferring to a lower height, with the front grab bar available and side guard in place 56% (64/115), CI[46%,64%] used the front bar and 19% (22/115), CI[13%,28%] could transfer to a lower height when using the front grab bar. When transferring to a higher height, with the front grab bar available, and the side guard, only 72 could transfer to a higher height and 51% (59/115), CI[42%,60%] used the front bar and 17% (20/115) , CI[12%,25%] could transfer to a higher height when using the bar. Although presented with the option to change the front grab bar height, subjects chose the same height for all the low height and high height transfers as they used when the side guard was not present.
Lateral grab bar use
The lateral grab bar was used least by subjects for the Adjustable gap protocol and most for the Side guard protocol. Lateral bar usage was not consistent for all transfers within a protocol ranging from 5% - 100% across all protocols and is likely influenced in part by alterations in the setup parameter (e.g. transferring higher may require usage while transferring lower may not).
Table 11 shows the number of subjects for each protocol who used the lateral grab bar for initial placement of their leading or trailing hands and in what percentage of their transfers. It can be noted that the lateral grab bar is used by more subjects when the transfer setup increases in level of difficulty (i.e. gap/height in combination or side guard).
Table 11 . Lateral grab bar use
| Protocol |
% Subjects |
% of Transfers used |
|
Height |
19% (25/116) |
32 ± 25% (5-100%) |
|
Gap |
11% (12/114) |
61 ± 32% (16-100%) |
|
Height/Gap |
41% (48/116) |
58 ± 32% (13-100%) |
|
Side guard |
37% (42/113) |
56 ± 34% (8-100%) |
|
Grab bar |
24% (28/115) |
37 ± 20% (8-100%) |
Table 11 Alternative Text Description: This table shows the number of subjects for each protocol who used the lateral grab bar for the initial placement of their leading or trailing hands and in what percentage of their transfers. The lateral grab bar was used by more subjects when the transfer setup increases in level of difficulty (i.e. gap/height in combination or side guard).
Table 12 summarizes the average clear space required for our subjects to position their WMD to perform a transfer in each protocol in terms of width, depth, and angle of approach (Figure 2). In the side guard protocol subjects tended to locate their wheelchair close to a perpendicular position with respect to the transfer station. The transfer setups that posed more barriers for our subjects such as height/gap, side guard, and side guard with front grab bar required more space for positioning the WMD.
Table 12 . Average clear space needed and WMD orientation for transfer for each protocol (mean ± standard deviation).
| Protocol |
Width |
Depth |
Angle (degrees) |
|
Height |
38.3 ± 11.6” |
40.7 ± 10.7” |
34±38 |
|
Gap |
39.9 ± 15.7” |
39.6 ± 12.2” |
34±38 |
|
Height/Gap |
39.8 ± 13.8 |
40.5 ± 11.3” |
29±31 |
|
Side guard |
38.7 ± 15.2” |
44.9 ± 18.1” |
37±35 |
|
Grab bar |
36.1 ± 13.0” |
47.9 ± 14.1” |
40±32 |
Table 12 Alternative Text Description: This table gives the average clear space needed and WMD orientation for transfer for each protocol (mean ± standard deviation). The transfer setups that posed more barriers such as height/gap, side guard, and side guard with front grab bar required more space for positioning the WMD.
Results comparison with current accessibility guidelines
Current accessibility guidelines for amusement park rides address recommendations for amusement ride seats designed for transfer in two places. First, it recommends a transfer height between 14 to 24” (35.6 to 61.0cm) and does not specify an allowable gap distance (2). Within this range, transfer surfaces are encouraged to be between 17 and 19” (43.2-48.3cm) high (2). Table 13 summarized the percentage of the subjects that could attain these heights for each protocol. Second, it requires that a minimum of 30” (width) by 48” (76.2x121.9cm) for a transfer with the WMD positioned parallel to the ride and assume a parallel approach for the transfer (0°) (2). Table 13 shows that the majority of WMDs (90%) could manage a 19” high surface with no gap and with or without the use of a front grab bar. Accessibility guidelines concerning handholds and grab bars where transfers are expected are not very detailed and are absent in the guidelines for amusement park rides. The height of a horizontal grab bar (parallel to the floor) is to be between 33”-36” (83.8 and 91.4cm) for water stalls, water closets, bathtubs, and bathrooms. Our subjects preferred the front grab bar height to be between 30-33” (76.2 and 83.8 cm).
Table 13 . Percentage of subjects in the sample that could attain the heights recommended in the ADA.
| Protocol |
14” high |
17” high |
19” high |
24” high |
|
Height |
43%(50/116) |
69%(80/116) |
90%(104/116) |
85%(99/116) |
|
Height/Gap (3.5” gap) |
30%(35/116) |
58%(67/116) |
76%(90/116) |
72%(84/116) |
|
Side guard |
27%(31/113) |
40%(45/113) |
43%(49/113) |
47%(53/113) |
|
Grab bar without side guard |
44%(54/115) |
71%(82/115) |
91%(105/115) |
88%(101/115) |
|
Grab bar with side guard |
29%(33/115) |
48%(55/115) |
57%(66/115) |
54%(62/115) |
Table 13 Alternative Text Description: This table gives the percentage of subjects in the sample that could attain the heights recommended in the ADA. The majority of WMDs (90%) could manage a 19” high surface with no gap and with or without the use of a front grab bar.
2. Accessible amusement rides - a summary of accessibility guidelines for recreation facilities. US Access Board; 2003.
Expert opinion on the current knowledge
Our review of the literature revealed a small number of studies that directly relate to the influence of transfer setup on performing independent transfers and thus points to a critical need for more studies in this area. All the studies identified also involved small groups of subjects and all of them included either subjects with SCI or unimpaired subjects except for one study (8) and thus a vast majority of them would not be generalizable to other populations who do independent transfers. There is not enough evidence in the literature or studies at the present time to determine the limits of setup that would make transfers in the built environment accessible to a majority of wheelchair users.
Transfer boards are a common aid used to facilitate transfers for those who have limited arm strength and/or situations where the height differential between the initial and target seats or gap difference is too large for them to negotiate without assistance. As the latter is a function of environment, we hoped to find studies that addressed the use of transfer boards or other similar technologies for circumventing environmental barriers.
In addition to transfer aids, experts also felt none of the original research studies were relevant to the issue of constrained space available for transfers. This item was geared to identifying issues concerning transfers into/out of an airplane seat, amusement park ride, or motor vehicle, by which the individual has a limited space to position the feet or legs when moving over to or from the target surface.
All the studies were conducted in laboratory settings versus ‘real-world’ environments with experimental setups that appeared free from any barriers that would limit leg/foot placement. Proper positioning of the feet is believed clinically to be a very important consideration for setting up for a safe and efficient transfer (9, 10) and thus may be critical for space planning in public areas where transfers are expected.
Physical obstacles and barriers are commonly observed for transfers to and from airline seats (e.g. arm rest is fixed) and amusement park rides (e.g. ride side rail/guard is fixed). Boats, kayaks, and other sorts of recreational equipment pose a similar barrier to transfers. None of the research identified described how well individuals are able to overcome physical barriers in between the wheelchair and target surfaces. In our own observations we see individuals going around or over the top of obstacles (e.g. transferring onto the obstacle first and then down into the seat/surface). The later is an example of a scenario that was scored separately for the item ‘number of transfers to go from the initial location to the final destination’ which was another aspect of setup reviewers identified as lacking evidence. There is no evidence suggesting how large (e.g. how high, tall and wide) an obstacle can be and still be accessible to a majority of wheelchair users.
Another area lacking sufficient evidence concerns the location and characteristics of effective supports to aid with transferring. This item encompassed for example the use of handholds, grab bars, or other environmental fixtures designed to facilitate a transfer to a target surface.
8. Finley M, McQuade K, Rodgers M. Scapular kinematics during transfers in manual wheelchair users with and without shoulder impingement. clinical Biomechanics (Bristol, Avon). 2005;20(1):32-40.
9. Gagnon D, Koontz A, Mulroy S, Nawoczenski D, Butler-Forslund E, Granstrom A, et al. Biomechanics of sitting pivot transfers among individuals with SCI: A review of the current knowledge. Topics in SCI Rehabilitation. 2009;15:33-58.
10. Sisto S, Druin E, Sliwinski M. Spinal cord injuries: management and rehabilitation. St. Louis, Missouri: Mosby Elsevier; 2009.
Evaluation of transfers
Our results clearly indicate that height above and below WMD seat height, gaps and obstacles can pose serious transfer-related accessibility problems for WMD users. Based on the guideline criteria in Table 13 pertaining to transfer heights alone (e.g. no gap and no obstacle), 15% of the sample could not transfer to a surface 24” high or higher and 57% of the sample could not transfer to a surface 14” high or lower. Note that none of the subjects had WMD with seats lower than 17 in which explains the lower percentages of subjects who could transfer to the recommended maximum low transfer heights compared to the higher heights (Table 13). A majority of our subjects (92% of the sample, CI[86%,96%]) managed a height at 22” (51cm) with no gap in place which is more similar to their own seat height. Thus it follows that transfers are the easiest to achieve when the height of surface to transfer onto is at the same height as the WMD (seat height + cushion). This is consistent with other research results that have found that level transfers require less exertion of the upper limb (3, 4, 6) . Study results suggest that an element’s height should fall within a range of 19”-23” to include 88% and within 21”-23” to include 90% of our sample.
A 2” transfer step height was acceptable for 86% of our sample; while current guidelines for pools and spas say step heights up to 8” are acceptable (11). It’s important to note that the step height in this study was a calculated value determined by subtracting the WMD seat height from the maximum (or minimum) target surface height to obtain a relative height difference. The 8” step in the pool/spa guideline refers to the height difference between two flat, step-like smooth surfaces and the wheelchair is not part of the transfer process. These types of transfers were not evaluated in our study. A future study is being developed to further evaluate transfer step possibilities (e.g. design features) for various kinds of transfer elements (e.g. amusement park rides) and allowances (e.g. height differences for multi-step or multi-tiered transfers).
Although gap has not been researched specifically (12), it is intuitive that the closer one is to the surface the easier it will be to move your body across. Our results also showed that fewer subjects were able to attain larger height differentials with a gap in place as compared to the setup without the gap. Therefore, attaining transfers at different heights than the WMD seat height across a gap is even more complicated.
Our results also showed that in terms of minimum space required for the transfer, the guidelines are insufficient (Table 12). Mainly because our subjects positioned their device at an angle instead of the parallel approach the guidelines suggest as well as the likelihood that today’s WMD’s vary more in size (13). ADAAG guidelines for pools and spas have recognized that people do not necessarily transfer parallel to the transfer target and suggest a clear deck area of 60” by 60” for transfer walls (11). This area could better accommodate our results’ mean plus one standard deviation of the area needed for our sample.
Introducing the side guard obstacle posed a significant barrier to transfer greatly reducing the number of subjects who were able to attain transfers at any height and/or gap. Despite the absence of recommendations regarding obstacles for transferring in the recreational facilities, guidelines for aircraft transportation for wheelchair users recognize that when the seat has a fixed armrest transferring is further complicated but it does not specifically recommend that armrest should be able to pivot (14). ADAAG guidelines for pools and spas suggest that if the lift seat has armrests, these need to be able to pivot so people can transfer from/to their WMD and the lift more easily (11). Our data suggest that adding a grab bar in front of the transfer seat helps to overcome a 6” obstacle and thus might be a worthwhile design criteria to include in future revisions of the guidelines. When the front grab bar was added in conjunction with the side guard, it was used more often but it did not help as many subjects to attain a higher or lower transfer compared to using the front bar without the obstacle in place. There was a high frequency of lateral grab bar use and front grab bar/lateral grab bar together upon initial hand placement. However, a decreased frequency of the use of the lateral bar was found in the grab bar protocol due to increased frequency of front bar use. Bars and the side guard were used often for repositioning the trunk and buttocks onto the platform after landing however the frequency of which these bars were used for this purpose was not documented.
Accessibility guidelines concerning handholds and grab bars where transfers are expected are not very detailed in general. Details are absent in the guidelines for amusement park rides and briefly referred to in the play area guidelines which suggests that transfer elements should have open sides (or an open side), back supports, and hand supports to help facilitate easy transfer and access (15). There is a general recommendation regarding the height of a horizontal grab bar (parallel to the floor) to be between 33”-36” (83.8-91.4cm) for water stalls, water closets, bathtubs, and bathrooms. Our study suggests that for a horizontal grab bar mounted in front of the element, the ideal height is between 30”-33” (76.2-83.8cm) high. One reason for the difference in heights between our study and the guidelines could be how the grab bar is used. In our study, we noted grab bar use for the initial hand placement and when the front bar was part of the set up it was used much more for this purpose than the lateral bar (e.g. this is the reason for the drop in Table 11 results for lateral bar use in the front grab bar protocol). Bars mounted horizontally on the side of the element may be used more to help with making adjustments onto the element once the initial transfer has occurred. As our subjects had to enter the station from the side (versus the front) the front bar was a closer handheld to use as opposed to reaching over to the lateral bar. Because the transfer occurs initially from a seated wheelchair position, a lower bar may help users gain the leverage necessary for lifting the body over to the new surface and back. The next phase of study will investigate further the usefulness of different type of handhelds and grab bar positioning during transfers.
Many studies have evaluated current accessibility guidelines in terms of space for maneuverability and finding them insufficient for current devices sizes (16-18) . These design parameters of the standard should be revised to reflect the setup of current WMD users as devices have changed since the standards were created in the 1970s. In 25 years, many changes have occurred in WMD users demographics and body sizes, as well as equipment characteristics (13). Equipment characteristics include increased use of positioning systems (e.g. tilt, recline, or combination which increases the effective length of the WMD), use of pressure-relieving cushions, and the availability of a wider range of wheel sizes (13).
3. Nyland J, Quigley P, Huang C, Lloyed J, Harrow J, Nelson A. Preserving transfer independence among individuals with spinal cord injury. Spinal Cord. 2000;38(11):649-57.
4. Gagnon D, Nadeau S, Noreau L, Eng J, Gravel D. Trunk and upper extremity kinematics during pivot transfers performed by individuals with sipanl cord injury. Clinical Biomechanics (Bristol, Avon). 2008;23(3):279-90.
6. Gagnon D, Nadeau S, Gravel D, Noreau L, Lariviere C, McFadyen B. Movement patterns and muscular demands during posterior transfers toward an elevated surface in individuals with spinal cord injury. Spinal Cord. 2005;43(2):74-84
11. Accessible pools and spas - a summary of accessibility guidelines for recreational facilities. US Access Board; 2003.
12. Koontz AM, Toro ML, Kankipati P, Naber M, Cooper RA. An expert review of the scientific literature on independent wheelchair transfer. Disability and Rehabilitation. 2011.
13. Steinfeld E, Maisel J, Feathers D, D'Souza C. Anthropometry and standards for wheeled mobility: An International Comparison. Assistive Technology. 2010;22:51-61.
14. Guidelines for aircraft boarding chairs. Washington DC: US Access Board 1988 [cited 2011 June 22]; Available from: http://www.access-board.gov/research/aircraft-boardingchairs/aircrarft-boarding.pdf.
15. Accessible play areas - a summary of accessibility guidelines for play areas. US Access Board; 2005.
16. Dutta T, King EC, Holliday PJ, Gorski SM, Fernie GR. Design of built environments to accomodate mobility scooter users: part I. Disability and Rehabilitation: Assistive Technology. 2011;6(1):67-76.
17. King EC, Dutta T, Gorski SM, Holliday PJ, Fernie GR. Design of built environments to accomodate mobility scooter users: part II. Disability and Rehabilitation: Assistive Technology. 2011;6(5):432-9.
18. Koontz AM, Brindle E, Kankipati P, Feathers D, Cooper RA. Design features that affect the menueverability [sic] of wheelchairs and scooters. Archives of Physical Medicine and Rehabilitation. 2010;91:759-64.
Study limitations
There are several limitations to this study worth noting. A large number of our subjects were veterans who participated in organized sports-related events however we have found that their daily activity levels apart from the time of the event do not differ from adult WMD users who live in community (19). If comparing the demographics of our sample to LaPlante et al (2010) who reported subject demographics among adult wheelchair users using data obtained by the US Census Bureau we find some similarities and some differences (Table 14). It is important to note that the LaPlante (2010) statistics are inclusive of full-time, part-time WMD users and those who rely on human assistance for wheeled mobility. The demographics of our sample resemble closely other studies that have specifically targeted independent mobility users thus further supporting the external validity of our study. For instance, a study that researched minimum space requirements for WMD maneuverability enrolled the majority of their subjects with spinal cord injury followed by central nervous system disorders ( multiple sclerosis, cerebral palsy, and spina bifida) (18). Similarly, a pilot study that investigated environmental barriers and facilitators for wheelchair users had the majority of its subjects with spinal cord injury followed by multiple sclerosis (20). Another study researched the effect of cross-slopes on the mobility of manual wheelchair users and also reported the majority of their subjects having spinal cord injury followed by multiple sclerosis, cerebral palsy, spina bifida, and amputations (21).
The number of handhelds, their positioning, and how they were used throughout the transfer process were not comprehensively studied. The lateral grab bar was at a fixed height, diameter, and length and always present on the station. Only one front grab bar of variable height was introduced as an optional handheld but its horizontal distance from the platform, diameter, and length was fixed. Its unclear what changes in the ‘fixed’ parameters could further aid users in the transfer process.
Table 14. Comparison between WMD users demographics reported by LaPlante (2010) and our study’s subjects demographics.
| Demographics characteristic |
Our sample |
LaPlante (2010) (22) |
|
Mobility device |
|
|
|
Manual wheelchair |
72% |
82.7% |
|
Power wheelchair |
24% |
9% |
|
Scooter |
4% |
8.3% |
|
Gender |
|
|
|
Male |
80% |
39% |
|
Female |
20% |
61% |
|
Age |
|
|
|
18-24 |
12% |
6.4% |
|
25-64 |
75% |
37.7% |
|
>65 |
13% |
55.9% |
|
Race |
|
|
|
Caucasian |
68% |
73.7% |
|
African American |
26% |
12.5% |
|
Hispanic |
3% |
7.9% |
|
Asian Pacific Islander |
2.5% |
1.9% |
|
Other |
- |
3.9% |
|
Disability causing use of WMD |
|
|
|
Paraplegia |
45% |
3.6% |
|
Cerebral palsy |
9.2% |
3.1% |
|
Absence or loss of lower extremity |
9.9% |
3.7% |
|
Multiple sclerosis |
8.3% |
5% |
|
Stroke |
1.7% |
11.1% |
|
Arthritis or rheumatism |
1.7% |
13.4% |
|
Orthopedic impairment of lower extremity |
1.7% |
3.6% |
|
Othera,b |
22.5% |
56.5% |
a Refer to Table 1 for Other type of self-reported disability in our sample
b Other in Laplante et al (2010) include diabetes, heart trouble, lung or respiratory problems, high blood pressure, blindness or vision problems, broken bone/fracture, cancer, senility/dementia/Alzheimer’s, kidney problems, mental or emotional problem, deafness or hearing problems, mental retardation and others which constituted 24.5% of the 56.5% and were not described in the article.
Table 14 Alternative Text Description: This table gives the comparison between WMD users demographics reported by LaPlante (2010) and our study’s subjects demographics. There are many similarities in the demographics between the two studies.
18. Koontz AM, Brindle E, Kankipati P, Feathers D, Cooper RA. Design features that affect the menueverability [sic] of wheelchairs and scooters. Archives of Physical Medicine and Rehabilitation. 2010;91:759-64.
19. Tolerico ML, Ding D, Cooper RA, Spaeth DM, Fitzgerald SG, Cooper R, et al. Assessing mobility characteristics and activity levels of manual wheechair users. journal of Rehabilitation Research and Development. 2007;44(4):561-72.
20. Meyers AR, Anderson JJ, Miller DR, Shipp K, Hoenig H. Barriers, facilitators, and access for wheelchair users: substantive and methodologic lessons from a pilot study of environmental effects. Social Science & Medicine. 2002;55:1435-46.
21. Souza A, Teodorski E, Sporner M, Cooper RA, editors. Effects of cross slopes on the mobility of manual wheelchair users. International Seating Symposium; 2010; Vancouver, CA.
22. LaPlante MP, Kaye HS. Demographics and trends in wheeled mobility equipment use and accessibility in the community. Assistive Technology. 2010;22(1):3-17.
Future Work
Bars and the side guard were used often for repositioning the trunk and buttocks onto the platform after landing however their use for this purpose was not documented. Grab bars and handhelds placed in other locations (e.g. in the front, on the sides, overhead, or to the element itself) could have enabled more successful transfers. The side guard although intended to serve as an obstacle to the transfer was sometimes used to facilitate getting in and out of the station. Future studies should look into the effects of variable ‘side guard’ widths, heights, contours and shapes to see if it such as structure could act more as a benefit versus a hindrance to the transfer. The next phase of study will research alternative hand placement options for both initial hand placement and repositioning upon landing on the target surface.
Only adult aged WMD users were studied and the sample consisted of a limited number of women and scooter users. The next phase of study will include children, more women, and scooter users. There is a lack of information about multi-step or multi-tiered transfers and how they can facilitate a barrier free or more level transfer for certain types of transfer elements (e.g. playground equipment, amusement park rides, medical diagnostic equipment) or places where transfers are expected (e.g. boat docks, airliners, etc.). A workshop and/or discussion panel with stakeholders (i.e. consumers, therapists, manufacturers, researchers, designers and Access Board members) is being planned to determine 1) what efforts should be made to mine the data gathered in the first phase to look at other transfer issues and 2) what other critical issues need to be addressed through research and design development in this area.
User Comments/Questions
Add Comment/Question