The Impact of Transfer Setup on the Performance of Independent Transfers: Phase I Final Report
Chapter 2: Methodology
Expert opinion on the current literature
Scientific literature databases were searched until June 2009 using 43 keywords resulting in 339 articles. These were internally reviewed and narrowed to 41 articles which were formally assessed by thirteen external experts. Articles that 80% or more of the reviewers scored as moderately or highly relevant were included in the results. Titles and abstracts of the articles were reviewed internally by two experts with at least four years of direct clinical and research experience working with full-time wheelchair users. Articles that both experts agreed were relevant to the performance of independent wheelchair transfers were selected for the next step of review. Thirteen external reviewers who are collaborators and work in the assistive technology and/or the rehabilitation field were invited to participate in a study to formally evaluate the remaining studies. Two reviewers held at minimum a bachelor’s degree, seven reviewers master’s degree, one was a physician and three held PhD degrees. All the reviewers had greater than five years of clinical research and/or practical clinical experience. The study was approved by the University of Pittsburgh Institutional Review Board.
External reviewers were sent a cover letter that described the purpose of the study and asked them to score each of the articles identified by the internal reviewers using a scoring sheet specifically devised for this study (Appendix 1).
Subjects
The target sample required wheeled mobility device users who lived in the community and were able to transfer independently (with or without a transfer board) and who represent a broad spectrum of disabilities. Subjects were eligible to participate if they (1) were at least 18 years old, (2) able to independently perform a transfer to/from a WMD with or without transfer board, (3) owned a WMD, and (4) had been using the WMD for at least one year. Subjects were excluded from the study if they had (1) significant upper extremity pain or injury that would inhibit the ability to perform transfers (2) active or recent history of pressure sores pressure sores.
Subjects were tested at the 24th National Disabled Veterans Winter Sport Clinic in Snowmass Village, Colorado during March 2010; at the 30th National Veterans Wheelchair Games in Denver, Colorado during July 2010; at the Hiram G Andrews Center in Johnstown, Pennsylvania during November 2010 and March 2011; during the US Access Board Meeting in Chicago, Illinois during September 2010; at the Human Engineering Research Laboratories in Pittsburgh, Pennsylvania between June 2010 and April 2011; and at H. John Heinz III VA Progressive care center in June 2011.
Measures and Procedures
A custom-built modular, transfer station was designed and built and consisted of a height adjustable platform capable of a range between 10” to 29” with increments every inch (25.4-73.7 cm in 2.5 cm) with a fixed backrest 17” wide by 25” high (63.5x43.2 cm) and a 95° recline; a lateral grab bar (fixed height of 32” or 81.3 cm) and allows for attaching/detaching side guards (e.g. obstacle to transfer) and an optional front grab bar of varying height (Figure 1) of 19”-38” (48.3-96.5 cm) with increments every 2” (5.1 cm). The grab bars’ diameter is 1.5” (3.8cm). The space for the legs and feet has a fixed dimension of 14.5” deep by 22.5” wide (36.8x57.2cm).
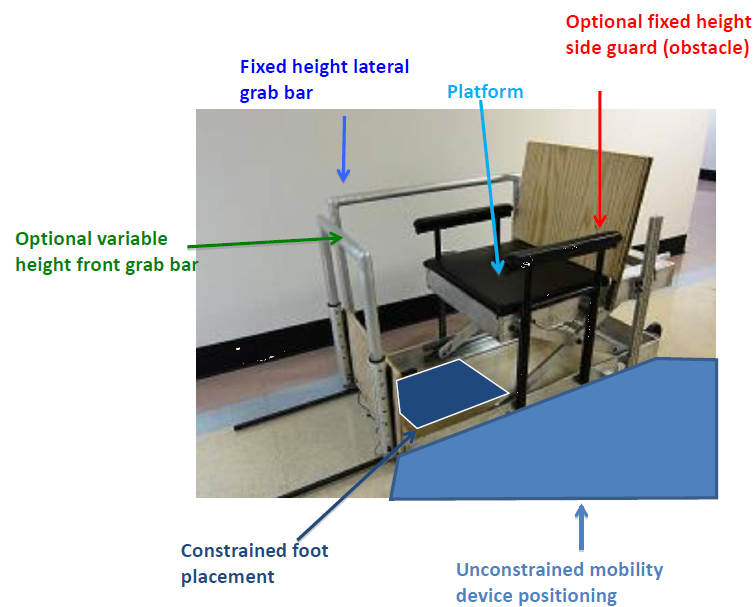
Figure 1 . Custom-built transfer station with the front grab bar, lateral grab bar, side guard, feet space, and space for WMD positioning highlighted.
For the initial setup, the platform was adjusted to be level with the subject’s WMD seat, with no side guard or front grab bar in place. The subjects were asked to position themselves next to the platform as they normally would to prepare for a transfer. Angular orientation and linear distances of the WMD with respect to the front most corner of the platform were recorded (Figure 2). Each subject was asked to perform a transfer from their WMD to the station and back to their WMD. Grab bar(s) use was noted. Next, they were asked to perform five protocols in random order. Subjects were asked to exercise sound judgment in performing the transfers and to only do transfers they felt comfortable and safe doing. Subjects were spotted in the event they would begin to slip/fall during a transfer in which the case the transfer was declared ‘unattainable’. After each transfer in each protocol, changes made to device positioning (x, y, α, Figure 2) and leading/trailing hand placement were recorded. The angle between the WMD and the transfer station is defined from 0°-180°. When the WMD is parallel to the transfer station and the subject is facing towards the front of the station the angle is defined as 0° and when the WMD is parallel to the transfer station but the subject is facing towards the back of the station the angle is defined as 180°.
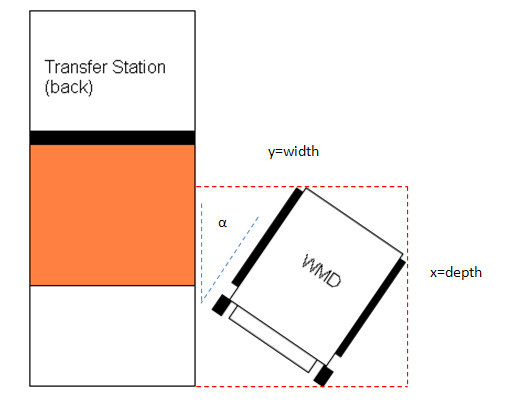
Figure 2 . WMD position measures taken to calculate the overall space needed to transfer
Adjustable height protocol: From initial setup, only the height of the platform was adjusted incrementally: higher (Figure 3) and lower than the subject’s seat. The amount of vertical distance that the seat was raised/lowered each time depended on the subject’s perceived and observed transfer abilities. The maximum and minimum heights the subject could transfer to/from the platform were recorded. As WMD seat heights differed among subjects, we also computed the difference between their seat height and the absolute maximum and minimum height they attained to calculate height differentials.

Figure 3 . Subject transferring to the transfer station set at a higher (left) and lower (right) height than the wheelchair
Adjustable gap protocol: From initial setup, just the horizontal distance between the WMD and platform was incrementally increased by placing plywood blocks of 3.5” (8.9cm) width between the transfer station and the WMD (Figure 4). The platform height remained level with their WMD seat height. The amount of horizontal distance increased each time again depended on the subjects perceived and observed transfer abilities. The maximum horizontal distance the subject could transfer to/from the platform was recorded.

Figure 4 . Person transferring with a 7in gap and the transfer station height at level with the wheelchair
Adjustable height/gap protocol: From the initial setup, a gap separating the device and platform was introduced with the plywood blocks of 3.5” (8.9cm) and then the height of platform was adjusted incrementally higher/lower (Figure 5). This procedure was repeated until the largest horizontal distance was reached. The maximum and minimum heights attainable with the largest horizontal distance were recorded.

Figure 5 . Subject transferring with a 7in gap and the transfer station higher than the wheelchair.
Side guard protocol: From initial setup, two side guards adjusted 6” (15.2 cm) higher than the subject’s WMD seat were attached, and subjects were asked to perform a level height transfer. Then the height of the platform was adjusted incrementally in height: higher and lower than the subject’s seat and the maximum transfer heights high/low that were attainable were recorded (Figure 6). Then from initial setup, the horizontal distance between the wheelchair and platform was incrementally increased and the maximum attainable gap distance was recorded. For all transfers with the side guard, side guard height was adjusted to be 6” higher than the WMD seat when the platform was level or lowered and 6” above the platform height when the platform was raised.

Figure 6 . Subject transferring with the side guard in place and the transfer station higher than the wheelchair
Front grab bar protocol: From the initial setup, an adjustable height grab bar was placed in front of the platform which enabled an additional optional handheld to assist with transferring to/from the platform. The horizontal distance between the center of the grab bar and the mid-center, front edge of the platform was 13.5”. Two conditions in random order were tested: 1) front grab bar and no side guard and 2) both front grab bar and side guard present in the setup. Subjects first performed a level height transfer in each condition and afterwards performed the variable height portion of the protocol as described previously (e.g. Adjustable height protocol). For each condition (e.g. grab bar with side guard and grab bar without side guard), subjects were asked to select their preferred grab bar height for both 1) transferring to lower heights and 2) transferring to higher heights than their WMD seat height. The preferred grab bar height was measured between the floor and the top of the grab bar surface. Maximum and minimum heights attainable, front grab use, and grab bar heights for each the lower-height and higher-height transfers were recorded.

Figure 7. Subject transferring with the side guard and front grab bar in place and the transfer station higher than the wheelchair
Data analysis
The number of subjects that attempted to perform each protocol and the number of subjects that were not able to attain the transfer(s) with that configuration are reported for each protocol. Descriptive statistics (e.g. means, medians, frequencies, standard deviations) of the data were calculated for the subjects that were able to attain the transfers in each protocol. Population proportion confidence intervals (CI) were determined at 95%. We compared our results with the current accessibility standards.
User Comments/Questions
Add Comment/Question