2.2 Key Measurement Variables and Procedures
We selected measurement variables and procedures for measurements based on advice provided by experts in anthropometry and ergonomics, human modelers, architects and designers, and clinicians.
The measurement variables include the following:
1. Demographic information and wheelchair description: Approximately 30 variables recorded with a checklist, along with digital still photographs of the user and mobility device.
2. Body and wheelchair dimensions: Approximately 125 locations of body and wheelchair points recorded in three dimensions.
3. Reaches and lifts: One-handed maximum reaches recorded at 5 different heights in three different directions for up to four different weight conditions (maximum of 60 reaches total).
4. Maneuverability: Four tasks related to propulsion in confined spaces.
5. Grip Strength: Three repetitions of maximal power grasp recorded for two different upper extremity postures and three repetitions of maximal pinch grip for two types of finger posture (lateral and thumb-forefinger pinches) (12 measurements total).
6. Door use: The level of observed effort was rated as participants used three different doors.
2.2.1 Demographic Information
A survey, checklist and photography were used to capture the demographic and wheelchair characteristics for each WhMD user. Demographic variables included: gender, age, disability status (category), years with the disability, and years using the mobility aid. Key variables associated with the mobility aid included device type (e.g., power chair, scooter), and within each type: make, model, age, armrests, footrests, drive wheels, controller, seat support surfaces and overall condition of the seating surface. A checklist was used to evaluate these device attributes (see Figure 2‒1). Digital photographs of the user and device were taken from the front and side views to document the wheelchair accessories and configurations of WhMD user.
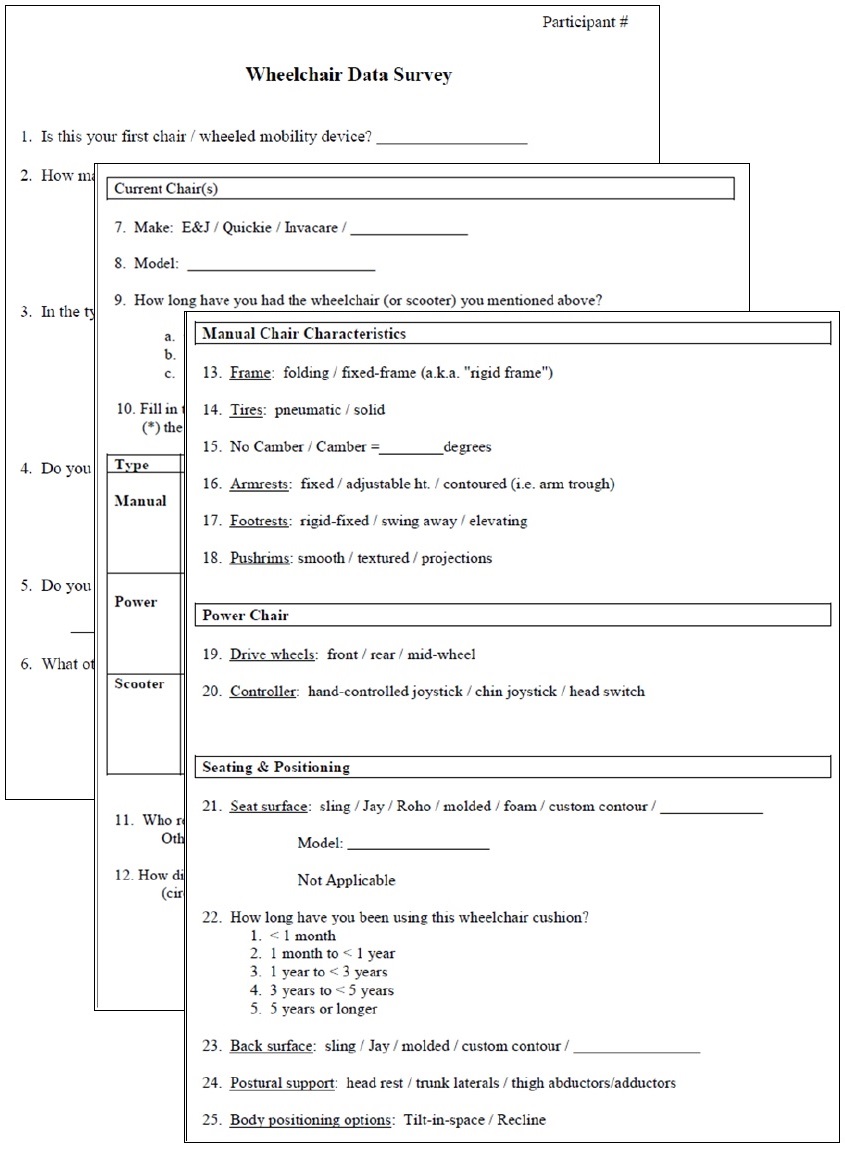
Figure 2-1. Portions of the checklist used to evaluate wheelchair characteristics
2.2.2 Structural Anthropometry (i.e. Body and WhMD Dimensions)
A three-dimensional (3-D) electromechanical probe (i.e. FaroArm, Faro Technologies Inc.) was used to record the 3-D location of body and WhMD device points (Figure 2‒2). The 3-D points were used to estimate body and WhMD heights, widths and depths and to construct static 3-D digital human models of WhMD users.
Figure 2‒2. Data collection with an electromechanical probe allows quick and accurate measurement of the widths, heights and depths of the body and mobility device characteristics.
The 3-D measurements required the measurement of reference points and planes, as well as the measurement of key body and WhMD points with respect to the environment. The IDeA Center has developed a detailed manual that defines each of the points in 3-dimensions, includes illustrations and explains applications for each of the points (Feathers et al., 2004). The reference points and planes, body points and WhMD points, and some of their application are listed in Tables 2‒1 and 2‒2.
Table 2‒1. Wheelchair and environment reference points and planes, and uses.

[Click image above to view HTML version]
Table 2‒2. Body points and important anthropometric dimensions associated with each point.

[Click image above to view HTML version]
2.2.3 Functional Reach
One-handed reach and lift capability data made at different heights, angles and object weights were collected in 3-D. Determining an individual’s 3-D reach envelope required that the reach envelope be measured relative to certain environmental, wheelchair and personal features (e.g. 3-D envelopes measured relative to a point on the floor, forward most portion of a person or wheelchair and/or from a reference point on wheelchair’s arm support surfaces). Data can be presented in 3-D, in the form of 2-D charts along key planes (e.g. sagittal plane to represent forward reach abilities), or described for a standard reach (e.g. maximum forward reach from a reference point).
The one-handed lifting tasks required individuals to move weighted cylinders that were empty or weighted with filler. Cylinders of 75 mm (3 in.) diameter were chosen because they required participants to use one-handed power or lateral pinch grasps, which are commonly used to hold and manipulate products. The size of the cylinders was held constant across conditions and participants. The four weight conditions were no weight, 1 lb, 3 lb and 5 lb.
Those individuals unable to grasp and/or lift any of the cylinders above shoulder height did not complete the reaches. Further, if a particular weighted canister could not be lifted above shoulder height then reaches involving that particular weight were avoided for reasons of participant safety.
Reaches and lifts were completed in 15 different directions (3 different angles of asymmetry from the orientation of the WhMD at 5 different heights). The angles of asymmetry included 0, 45 and 90-degrees from the sagittal plane that passes through the acromion process on the individual’s dominant side (i.e. forward, asymmetric and side reaches, respectively). The five heights were normalized to the individual's vertical reach capabilities so that reaches were performed at, above and below shoulder height.
Three-dimensional reach data were collected with the electromechanical probe (FaroArm, Faro Technologies). Use of the electromechanical probe required manually digitizing the 3-D location of the maximum reach point after the cylinder was positioned (Figure 2‒3). The point data were used to measure reach distances from reference points (e.g. maximum forward reach from the front of the WhMD, or maximum side reach from the lateral-most point of the WhMD), and construct reach envelopes that illustrate the reaching capabilities of the sample in 2-D and 3-D space.
A computation procedure was developed for performing analyses on reaches that involved combining 3-D reach information from the measured WhMD users in relation to a common reference plane. For instance, a vertical plane at the anterior-most point was used a reference to analyze forward reaches. This is similar to a wheelchair occupant facing a wall such that the forward-most aspect of their foot and/or wheelchair was touching the wall. Likewise, a vertical plane at the lateral-most point was used as a reference for analyzing lateral reaches, similar to a situation where a wheelchair occupant were right alongside a wall.
The percentage of WhMD users able to reach to or beyond a particular reference plane (either forward or lateral) was then computed. The data were analyzed in 100 mm (4 in.) increments from the floor. The reference planes could also be moved away or towards the occupant to simulate different obstruction depths to estimate the relative increase or decrease in reach capability. It should be emphasized that our data depict, in percentages, the reaching capabilities of only those individuals who could grasp and lift a particular cylinder above shoulder height.

Figure 2‒3. Participants moved cylinders in 3 different directions at 5 different heights. Shown are forward reaches for two different heights. The electromechanical probe is used to record the 3-D location of the maximum reach distances from body and wheelchair reference points.
2.2.4 Maneuverability
WhMD users were video recorded while completing the following tasks:
• 90-degree turn,
• 180-degree turn with no restrictions on length of the maneuver,
• 180-degree with a center barrier,
• 360-degree rotation within a space with four walls.
The tasks were performed in restricted space conditions with the maneuvering performed within the confines of temporary barriers that are made of cardboard. Widths of the restricted space were set at a minimum of 750 mm (30 in.) for the 90-degree turn, 750 mm (30 in.) passage width for the U-turn with a barrier, and 1300 mm (51 in.) for the 180-degree and 360-degree turning activities.
WhMD users were asked to complete the tasks without touching the walls. The separation between walls was increased at increments of 50 mm (2 in.) if passage through the mock environment was not cleared without touching the walls (Figure 2‒4).
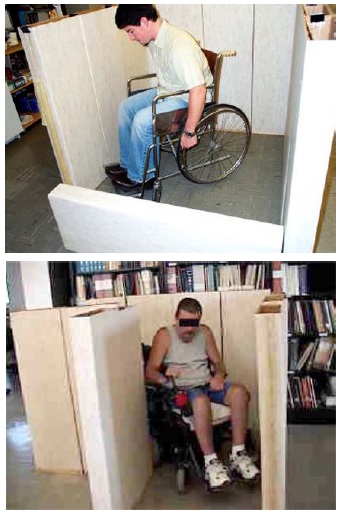
Figure 2‒4. Two examples of WhMD users completing restricted space experimental conditions.
2.2.5 Grip Strength
Four types of grip strength measurements for the dominant hand were assessed. These included a power grip with the elbow in full extension (i.e. shoulders flexed 90-degrees and upper extremity fully extended), power grip with the elbow flexed 90-degrees, lateral pinch (i.e. with the pinch gauge between the thumb pulp and the radial aspect of the forefinger), and thumb-forefinger pinch (i.e. with the pinch gauge between the tips of the thumb and forefinger). These measurements are important to the design of and/or standards development for some types of hand tools, hardware and electrical controls (e.g. scissors, some types of door latches, knob controls). Grip strength was recorded with manual hand and pinch dynamometers (Jamar, Inc). WhMD users were required to perform three maximal efforts in each of the four types of grips with their dominant hand, with the mean value considered as the maximal force value for analysis. Force measurements were not obtained for those WhMD users that were unable to perform a grip or exert a grip force, or declined from grip measurements (e.g. due to pain or discomfort in the hand). If the person could not complete all three force repetitions, force data for that particular grip was not included in the analysis.
Prior analysis of a subset of this data (D’Souza et al., in review) showed maximal power grip forces to be greater on average by approximately 1% to 5% with the arm in full extension as compared to with the elbow flexed 90-degrees on average across gender and mobility device type. In light of this marginal difference, only the power grip data measured with the elbow flexed 90-degrees along with data on pinch grips are included in this report. Additional analyses of this data to study potential differences in grip strength capabilities by age and medical condition that may clinical relevance have also been reported (e.g. Joseph et al., 2010).
2.2.6 Door Use
Our study of door use had three main objectives all intended to provide groundwork for future studies aimed at design guidelines and standards that would make doors more accessible to WhMD users:
1. Identify door use tasks that present WhMD users with the most difficulty,
2. Evaluate how different aspects of door design effect door use difficulty, and
3. Identify which WhMD user groups experience the greatest difficulties with doors.
The door use tasks required the use of three different doors in the building housing the IDeA Center. Trials in both directions were performed (i.e. from push and pull sides) using a forward approach. Each door presented different types of challenges to WhMD users. The door characteristics are summarized in Table 2‒3.

[Click image above to view HTML version]
For each trial, use of the door was divided into six task components: Opening Maneuver, Operating Latch, Opening, Through Passage, Closing Maneuver and Closing (See Figure 2‒5). For each phase, the level of difficulty experienced during each task was assessed using a 4 point scale and definitions previously developed and tested by Danford and Steinfeld (1999):
1. Minimal effort: The task was performed successfully on the first attempt, without an expression of frustration, smoothly without interruption, and in no more time than it would take for a member of the general population.
2. Moderate effort: The task was performed successfully on the first attempt, with no more than a brief expression of frustration and infrequent pauses or slight difficulties that increase the task time slightly as compared to a member of the general population.
3. Maximal effort: The task was performed successfully after multiple attempts, often with some expression of frustration and frequent pauses or difficulties that dramatically increases task time as compared to a member of the general population.
4. Impossible: The task was not performed successfully or there was a refusal to complete the task.
5. Blocked View: The effort could not be assessed due to visual obstruction between observer and WhMD user (e.g., door in the way for closing maneuvers, the WhMD user’s body orientation with the observer prevents an assessment).
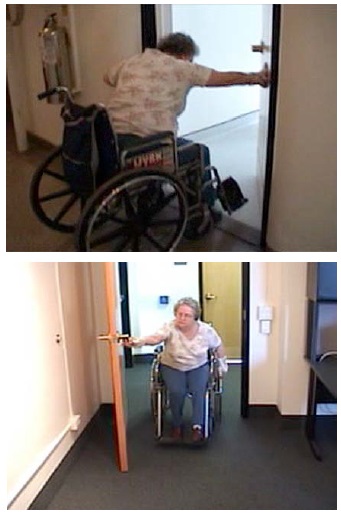
Figure 2‒5. Two examples showing physical requirements of door use for two of the doors used by WhMD users.
User Comments/Questions
Add Comment/Question