Access for All: Five Years of Progress - A Report from the Department of Justice on Enforcement of the Americans with Disabilities Act
II. ENFORCING THE ADA PART 2
5. Equal Access to Parks and Recreation
A local government's parks and recreation facilities play an important part in the life of a community and its members. Unfortunately, many parks and recreation facilities were built without accessibility in mind. Because of this, individuals with disabilities and their families often cannot participate in programs and activities offered at such places as public parks, baseball and football fields, town pools, and county recreation centers.
Under federal regulations, when parks and recreation facilities are built or altered, they must comply with the ADA Standards for Accessible Design (ADA Standards), which require inclusion of features such as accessible parking spaces, routes, toilet facilities, public telephones, and spectator seating areas.37 For parks and facilities that were built or altered before the ADA Standards took effect, local governments usually must devise ways to make the programs and activities in those parks and facilities accessible to people with disabilities. If a local government decides to modify facilities to provide access to a recreation program or activity and has more than one facility available (such as when several ball fields are provided), only some of the facilities may need to be accessible.
As part of our Project Civic Access initiative, the Department routinely surveys parks and other recreation facilities to ensure that they are accessible to people with disabilities. Investigations have included reviews of parks, community centers, recreation centers, nature centers, skate parks, sports and fitness centers, public golf courses, docks, and other recreation areas. The Department has entered into approximately ninety settlement agreements to resolve issues found at such facilities. These agreements include provisions to make toilet rooms accessible, to provide accessible golf carts, and to make paths of travel to play equipment and sports fields accessible.38
The Department's work with communities across the country demonstrates that improving access to parks and recreation areas is important to the quality of life of people with disabilities and to their families and friends. Access to parks and other recreation areas and programs affects an individual's quality of life no matter where he or she lives, from Florida to Alaska and every community in between. For example, in 2002 the Department worked with the City of San Antonio, Texas, to identify ways in which the historic city's programs and activities could be made more accessible. Under the resulting settlement agreement, San Antonio agreed to make physical alterations to city-owned and operated facilities, buildings, and streets to ensure that individuals with disabilities, residents and visitors alike, could fully participate in the city's numerous recreational offerings.
This positive collaboration between the Department and the city has made a difference in the quality of life for everyone in San Antonio. Residents and visitors who use wheelchairs now can enjoy the city's famed Tea Pagoda in Brackenridge Park because the city installed appropriate ramps. Performances at the park's Sunken Gardens Theater can be enjoyed by all because the city constructed wheelchair-accessible seating locations throughout the theater. And families can plan gatherings at a community park with the comfort of knowing that the park's parking, picnic grounds, restrooms, and swimming pools are accessible to individuals with disabilities.

Accessible route to Elmendorf Park swimming pool, San Antonio, Texas.
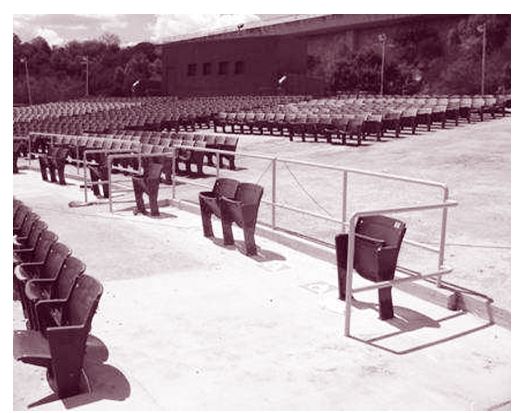
Wheelchair accessible and companion seating at the Brackenridge Park Sunken Gardens Theater, San Antonio, Texas
In July 2002, at a ceremony commemorating the twelfth anniversary of the ADA, the Department publicly recognized San Antonio's positive, ongoing approach to increasing access for all its citizens and visitors.39 Residents, too, have expressed excitement about the city's commitment to full participation for all. Donna McBee, who is blind, remarked on the stark difference the city's commitment has made in her life as a resident of San Antonio: "I first moved to the city in 1981 and would navigate the city streets with a cane. . . . I wasn't always certain of my safety when crossing the street. Since the passage of the ADA, access has improved greatly and mobility is much easier. So much has changed!"40
The City of Springfield, Missouri, was recognized as well at the 2002 ceremony for its efforts in complying with its Project Civic Access settlement agreement.41 Springfield's citizens have also recognized and appreciated the city's efforts to increase access at its many parks, including new accessible paths to playground equipment and picnic tables. For example, Margaret Trimble, a Springfield resident and self-described outdoors person, uses a walker because of a mobility impairment and often found her choices limited to those parks with the fewest obstacles.42 Ms. Trimble told the Department that she is pleased with the changes and added, "The more that parks and natural areas are accessible [the more it] helps families. I really enjoy being able to get down to the banks of a trout stream or being able to attend family and other group outings – wherever they are held."43

Twelfth Anniversary ADA Ceremony in July 2002 at DOJ with participants including Former Assistant Attorney General Ralph Boyd and Deputy Assistant Attorney General Loretta King
Communities with extreme conditions can encounter unique challenges in furthering the ADA's goal of full participation. For example, in Juneau, Alaska, fishing is a major recreational activity for tourists and citizens alike. Because of Juneau's extreme tides, providing docks at a slope that can be navigated by persons with mobility impairments is a difficult task. But, given the importance of fishing as a community recreational activity, Juneau was determined to build accessible fishing docks. Officials used state and federal money to build two accessible fishing piers, one in freshwater and one in saltwater. One dock is reinforced so that persons with mobility impairments can drive their vehicles out onto the dock, where a lift-off lip assists them as they transfer onto boats. In 2004, the Department reached a settlement agreement with Juneau, according to which the city also agreed to improve accessibility at several harbors, parks, and gyms, as well as at an ice arena, shipping dock, pool, museum, youth center, and visitor's center.44
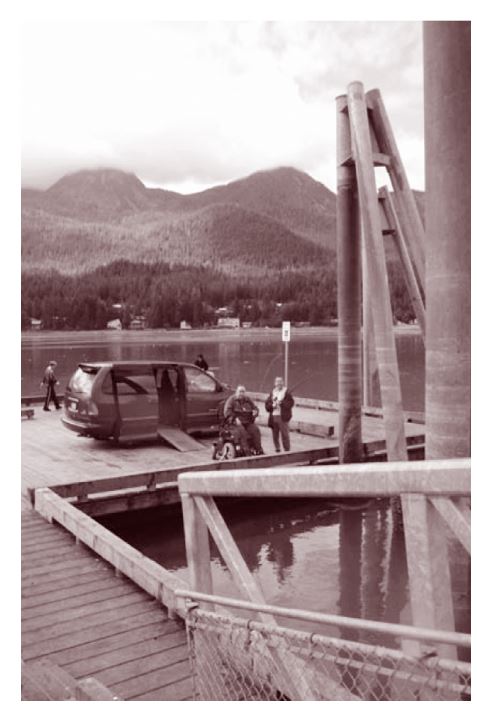
Accessible Fishing platform in Juneau, Alaska.
San Antonio, Springfield, and Juneau are just three examples of the many local governments that have already significantly improved access to parks and recreation programs as a result of Project Civic Access. Virtually all of the Project Civic Access agreements the Department has reached in the past five years have required cities and counties to begin work to make recreation facilities and programs more accessible to people with disabilities. For example, in 2005 the Department signed an agreement with Florence County, South Carolina, requiring the county to, among other things, improve access to five parks and its civic center.45 And this year, the Department reached a settlement agreement with Arlington County, Virginia, which requires Arlington to improve accessibility at eleven parks, four community centers, two recreation centers, a nature center, a skate park, and a sports and fitness center.46
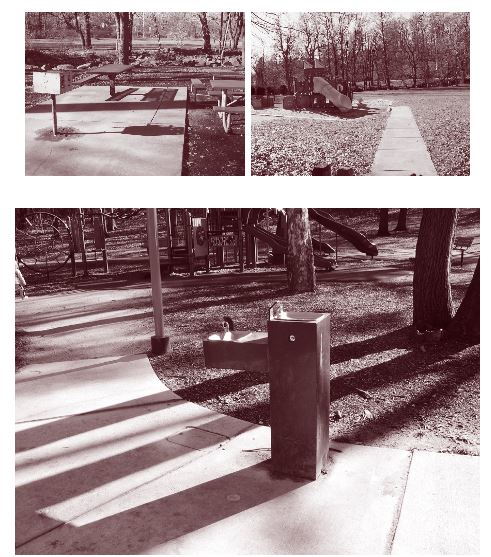
Accessible picnic table, route to playground equipment, and drinking fountain in Arlington County, Virginia.
Whether the fix is simple, such as extending a picnic table to allow an individual who uses a wheelchair to use it, or more complex, like providing access to docks in communities with tides, these solutions are essential to ensure that people with disabilities have the same opportunities as others to enjoy recreational facilities with their family members, friends, and colleagues. Equal access to parks and recreation is a mandate of the Americans with Disabilities Act. The Department will continue to make the enforcement of this mandate a priority along with enforcing equal access in other aspects of everyday civic life.
B. Ensuring Equal Health Care Access
Titles II and III of the ADA cover doctors, dentists, and other health care providers, as well as all hospital programs and services, including emergency room care, inpatient and outpatient services, surgery, clinic services, educational classes, and cafeteria and gift shop services.
Despite the ADA's mandate of equal treatment and accessibility, people with disabilities experience discrimination in a variety of manners in health care settings. For example, in 2001 the Department began an investigation of the Staten Island University Hospital in response to complaints filed with the Department alleging a range of accessibility problems: a separate entrance and separate waiting room for patients with developmental disabilities at its dental clinic, lack of accessible parking and accessible restrooms at its dental clinic, and lack of accessible equipment at its gynecological clinic. The Department negotiated a settlement agreement in 2003 requiring the hospital to resolve these problems and, in addition, to provide auxiliary aids and services for effective communication with people who are deaf or hard of hearing, to make reasonable modifications in policies and procedures as necessary to avoid discriminating against people with disabilities, to provide ADA training to staff, to notify the public of the hospital's obligations under the ADA, and to pay $8000 in civil penalties.47
The three most prevalent accessibility issues in health care settings are lack of effective communication, lack of accessible equipment and services, and refusal of care.
1. Effective Communication
Wherever patients with hearing disabilities interact with hospital staff, a hospital is obligated under the ADA to provide effective communication. The Department's agreements and consent decrees match the methods of communication and services or aids needed to effectuate communication with the abilities of the person who is deaf or hard of hearing and the nature of the communications that are required. For example, exchanging written notes or pointing to items for purchase will likely be effective communication for brief and relatively simple face-to-face conversations, such as a visitor's inquiry about a patient's room number or a purchase in the gift shop or cafeteria. Written forms or information sheets may provide effective communication in situations where there is little call for interactive communication, such as providing billing and insurance information or filling out admission forms and medical history inquiries.
However, in the past few years the Department has focused on ensuring that, for more complicated and interactive communications, health care personnel are aware that it may be necessary to provide a qualified sign language interpreter. Examples of such communications include discussion of symptoms between a patient and medical personnel; presentation by a physician of diagnosis and treatment options to patients or family members; communication with a patient during treatment, testing procedures, or rounds; group therapy sessions; or delivery of educational presentations.
In addition, under some circumstances, the Department's agreements and decrees have provided for an interpreter or other aid for a patient's family members who are deaf or hard of hearing. In United States v. Parkway Hospital, Inc., the Department filed a lawsuit in 2003 against Parkway Hospital, a private hospital in Queens, New York, because the hospital allegedly failed to provide a qualified sign language interpreter for Sarah Posner, an elderly deaf patient, or her husband, who is also deaf, during Mrs. Posner's extended hospitalization at Parkway. In addition, the Department alleged the hospital violated the ADA by imposing communication responsibilities on the Posners' grown children, who were expected to act as conduits for information between the family and hospital staff. Because of these failures, Mr. Posner allegedly was unable to obtain complete information about his wife's medical diagnosis, treatment, and prognosis. Under a consent decree approved by the United States District Court for the Eastern District of New York in 2004, the hospital was required to pay $125,000 in compensatory damages to the family of Mrs. Posner, who was then deceased, and to adopt sign language interpreting policies and procedures intended to ensure effective communication for deaf patients and their family members.48
The Department recognizes that enhanced and emerging technologies may allow health care providers to obtain qualified interpreters more quickly, economically, and efficiently 24 hours a day. For instance, providers may utilize video interpreting services whereby a qualified sign language interpreter appears via video from a remote location on a television-like screen. A health care provider opting for this approach, however, must take the necessary steps to ensure that the appropriate hardware and software are in place to support the system, and that staff understand how to operate and maintain the equipment. This is especially critical in the hospital setting. Where a hospital purports to utilize video interpreting services but does not provide the necessary administrative and operational support to ensure the system works, a patient with a hearing disability is denied his or her right to fully participate in health care decisions, and family members are shut out from communicating with the hospital about their loved one.
E-mail dated August 7, 2006, from Norman Posner, husband of Sarah Posner
For example, in 2006 the Department intervened in a private lawsuit, Gillespie v. Dimensions Health Corp., d/b/a Laurel Regional Hospital,49 brought by seven deaf individuals against Laurel Regional Hospital alleging a failure to provide appropriate auxiliary aids and services, including qualified interpreters, necessary to ensure effective communication for deaf patients or deaf family members, either in the emergency department or during hospitalizations. In that case, the Maryland hospital had an older system of video interpreting services available, but hospital staff allegedly had difficulty setting up and operating the system. The picture allegedly was, at times, too blurry for a patient to clearly distinguish the arms and hands of the video interpreters, and the video camera allegedly could not be adjusted for prone patients so that the interpreter and the patient could clearly see each other's hands, arms, and heads.
The allegations in the Laurel Hospital case illustrate the problems that can result when a hospital fails to take the necessary steps, through a video interpreting service or otherwise, to ensure effective communication. Hospitals often mistakenly use family members as interpreters in non-emergency situations and inappropriately rely on lip-reading for complicated medical communications – allegations the Department has also encountered in other cases in which it has been involved.50 In Laurel Hospital, the complainants alleged that the hospital failed to provide an interpreter for a deaf patient during hospitalization. The hospital allegedly did not attempt to communicate with the deaf patient in any way, but rather forced her hearing mother to function as a relay person, consecutively exchanging simplistic messages between her adult daughter and the hospital regarding her daughter's condition and treatment. The patient complained to the Department that her mother was often unable to communicate to her what hospital personnel had said, and that because her mother does not know sign language, the patient was forced, often unsuccessfully, to try to read her mother's lips. The patient said she felt frustrated, angry, and ignored by the hospital.
In 2006, the Department resolved the Laurel Hospital case through a comprehensive consent decree,51 which was modeled after several other agreements and decrees executed in the last few years,52 and which included detailed provisions for the implementation and administration of a program to ensure effective communication with persons with hearing disabilities. The consent decree required the hospital to continue to provide both on-site interpreters and interpreters appearing through video interpreting services where necessary for effective communication; to provide other auxiliary aids and services as necessary; to modify medical and intake forms to ensure that once a deaf or hard-of-hearing patient or family member enters the hospital, the hospital makes a communication assessment and, if necessary, a reassessment of the patient or family member; to maintain a complaint resolution/grievance procedure regarding the provision of auxiliary aids and services; and to train hospital personnel to accommodate the communication needs and preferences of deaf or hard-of-hearing patients and family members.
In addition, the Department required Laurel Hospital to satisfy specified performance standards for its video interpreting services regarding the quality and clarity of the televised video and audio, regardless of the body position of the patient, and to train hospital staff to quickly and easily set up and operate the system. The Department also made clear that, except in very limited instances, medical providers should not ask family members or other representatives to interpret for a person who is deaf or hard of hearing because of potential emotional involvement, considerations of confidentiality, and limited interpreting skills.
In United States v. Fairview Health Services,53 the Department entered into a consent decree settling a lawsuit alleging that Fairview Health Services failed to provide qualified sign language interpreters and services to deaf patients. Under the agreement, Fairview agreed to hire and make available one or more qualified sign language interpreters 24 hours a day, seven days a week, to provide effective communication at each of its five hospitals in Minnesota, and to pay $188,000 in damages to four complainants and $20,000 in civil penalties. Fairview will also rewrite its hospital policy and procedures affecting patients with disabilities, develop patient and visitor information and notices in forms that are accessible to deaf and hard-of-hearing patients, and conduct comprehensive training of hospital personnel. Similar agreements have been reached with Greater Southeast Community Hospital in Washington, D.C., St. Francis Healthcare in Wilmington, Delaware, and South Florida Baptist Hospital in Plant City, Florida.54
The Department has resolved complaints about other types of health care providers as well. For example, an eye surgeon doing business in New York City as Advanced Eye Care Associates advertised a free consultation for anyone considering laser vision correction. A man who is deaf called to schedule an appointment and advised the doctor's office that he would need a sign language interpreter at the consultation. He alleged that the doctor's office refused to pay for an interpreter, cancelled the appointment, and told the complainant that he was not a suitable candidate for laser eye surgery because he was deaf. Under the 2005 consent decree in United States v. Saimovici, Advanced Eye Care agreed to follow a policy of nondiscrimination on the basis of disability and to provide appropriate auxiliary aids, including qualified sign language interpreters, free of charge when necessary to ensure effective communication.55 The doctor also agreed to pay $3500 in civil penalties and $1500 in compensatory damages to the complainant.
In another case, a consulting psychologist in Oklahoma City, Oklahoma, who had been court-assigned to consult and evaluate family members involved in a divorce case, allegedly failed to provide an interpreter during an evaluation of a minor child who is deaf. The Department reached an agreement with the psychologist in August 2005 in which he agreed to provide individuals who are deaf or hard of hearing with appropriate auxiliary aids and services, to conduct an individualized assessment to determine which aid or service is needed, and to inform people with disabilities of the availability of auxiliary aids and services.56
A dental clinic in Indiana also entered into an agreement with the Department, resolving a complaint filed by a woman on behalf of her husband who is deaf. The complainant alleged that she requested a sign language interpreter when she called the clinic to schedule a dental appointment for her husband, who needed complex and extensive dental services, but the clinic refused her request. In the April 2006 agreement, the clinic agreed to adopt an effective communication policy and an effective communication assessment form, to post a sign in all of its ten dental offices informing patients that the clinic will provide qualified sign language interpreters when necessary, and to provide mandatory training to all of its employees about the ADA and its new effective communication policy.57
2. Accessible Medical Equipment and Facilities
The use of medical equipment is vital to the provision of medical care. Health care providers use diagnostic equipment to detect serious diseases at an early stage when such diseases are treatable. Unfortunately, the lack of accessible medical equipment and facilities denies health care to many individuals with disabilities. Necessary accessible medical equipment includes examination tables, examination chairs, scales, radiologic equipment (e.g., x-ray and MRI equipment), dental chairs, ophthalmology equipment, and any other equipment used in the medical context that are accessible to and usable by individuals with mobility impairments and other disabilities.
Many individuals with disabilities do not receive adequate medical treatment. For instance, many such individuals receive less comprehensive medical examinations than they should because they are unable to transfer to the proper examining table or chair or to use inaccessible equipment.
The increasing significance of diagnostic testing further underscores the importance of full and equal access to health care services for individuals with disabilities. Cervical and breast cancer rates have been reduced, due in large part to the critical role of preventive measures such as mammography and pap smear tests. These tools are essential in early disease detection, which often is the key to effective treatment and survival. Failure or refusal to perform such examinations and tests due to disability is discriminatory and can have grave consequences. The Department is committed to ensuring that, as the ADA requires, health care services, medical equipment, and diagnostic tests are accessible to individuals with disabilities.
For example, in 2005 Exodus Women's Center, which provides obstetrics and gynecology services to women in four different locations in Florida, entered into a settlement agreement with the Department.58 The agreement stems from a complaint filed by a woman who uses a wheelchair due to a neurological condition. The complainant alleged that, when she arrived for her appointment, Center staff told her that she needed to bring someone to assist her onto the examination table and refused to help her transfer. She left without receiving an important medical examination.
Under the terms of the agreement with the Department, Exodus Women's Center agreed to:
-
purchase an adjustable-height examination table for one office within two months of the agreement and a second table for another office within twelve months;
-
ask patients, when scheduling an appointment, if they will need any assistance, modification of policy, or auxiliary aid or service during the exam due to a disability; and
-
conduct ADA training for all of its medical and administrative staff, including teaching transferring techniques and providing sensitivity training on interacting with individuals with disabilities.
Another alleged failure to provide obstetrics and gynecology treatment involved the Obstetrics and Gynecology Clinic at Georgetown University Medical Center. In 2001, the Department and Georgetown entered into a settlement agreement after the Department received a complaint by a woman who alleged that Georgetown had failed to assist her with transferring from her wheelchair to an examination table when the sole adjustable table was not working.59 Georgetown agreed to pay a civil penalty of $10,000 and damages of $15,000 to the complainant.
When visiting doctors' offices, individuals with disabilities often face major obstacles due to simple things that people without disabilities would not even notice. For example, individuals with mobility impairments may not be able to get into examining rooms due to narrow doors, or they may not be able to maneuver within a room once they gain access. In addition, examination tables and chairs present some of the biggest obstacles for individuals who use wheelchairs or other mobility aids; transfer to an examining table or chair can be impossible without an adjustable table or mechanical lift. The Department's settlement agreement in 2005 with Dr. Robila Ashfaq, a solo practitioner in family medicine in Irvine, California, followed a complaint from a woman with paraplegia who used a wheelchair. She alleged that her husband assisted her onto the examining table during her first visit and that subsequent examinations were conducted in her wheelchair. The complainant further alleged that after she requested that the doctor borrow or purchase an adjustable examination table or lift to facilitate her transfer, Dr. Ashfaq stated that she could not provide an accessible table or lift due to budget constraints and discontinued treating the complainant as a patient.
"When I asked my physician to purchase an accessible exam table, or make some other kind of accommodation, she refused . . . I knew my rights and knew the ADA law backed up my request, so I contacted the Department of Justice and asked for help. They were very understanding, and the claim process was much simpler than I ever thought it would be. When the case was settled and my doctor purchased the accessible exam table, I felt like I had done something really important for others who had mobility issues, especially for women, because there are so few doctors that have them. It feels good to know that I not only helped myself, but helped others, as well."
- E-mail dated August 8, 2006, from Holly Bercik, Orange County, California
Under the terms of the agreement with the Department, Dr. Ashfaq agreed to:
-
purchase an accessible, adjustable-height exam table;
-
adopt a nondiscrimination policy;
-
attend training with her staff about ADA requirements; and
-
ask patients, when scheduling appointments, if they will need any assistance, modification of policy, or auxiliary aid or service during the exam due to a disability.60
In some cases, mammography equipment is literally out of reach of women who are unable to stand, and, in addition, many medical offices and hospitals do not have scales designed to weigh a patient while sitting in his or her wheelchair. Lastly, some facilities lack simple ancillary equipment (e.g., stabilizing elements on examination tables to prevent falling or leg supports for gynecological examinations) that would make otherwise inaccessible medical equipment fully accessible.
As part of its commitment to ensure fully accessible medical treatment for persons with disabilities, the Department entered into two of its most comprehensive settlement agreements under the ADA with Washington Hospital Center and Valley Radiologists Medical Group in November 2005.
Under the terms of the agreement, Washington Hospital Center agreed to:
-
create a minimum of 35 fully accessible patient rooms, with each including an accessible toilet room and an accessible shower (or access to one);
-
purchase adjustable-height beds for all of its accessible inpatient rooms;
-
ensure that each department has at least one accessible examination table that lowers to 17-19 inches from the floor to enable individuals
-
who use wheelchairs to transfer to the examination equipment;
-
survey all of the equipment in the hospital and purchase new accessible equipment needed to ensure that individuals with disabilities receive equal access to medical services, including an accessible examination table or chair in each hospital department that utilizes them;
-
implement a barrier removal plan; and
-
update hospital policies and train staff to address the needs of individuals with disabilities.61

- E-mail dated August 8, 2006, from Rosemary Ciotti, R.N., M.S.N.
The Department's agreement with Valley Radiologists Medical Group arose out of a complaint involving a woman who visited a radiologist's office for a full-body bone density x-ray. Because the woman uses a wheelchair, she allegedly was unable to transfer herself to an examination table without a mechanical lift, which the clinic did not have. As a result, the x-ray could not be performed.
Under the terms of the agreement with the Department, Valley Radiologists Medical Group agreed to:
-
purchase four mechanical lifts and eight transfer boards;
-
ask patients, when scheduling an appointment, if they will need any assistance or service during the exam due to a disability;
-
provide appropriate assistance and equipment at an appointment when requested; and
-
train all medical and administrative staff about the requirements of the ADA, the operation of the transfer equipment, and techniques for assisting individuals with mobility impairments with transferring to the exam table.62
3. Refusal of Care
Having access to health care is a fundamental part of American life. For some individuals with HIV, that access is compromised by health care professionals who refuse to treat those with HIV. The Department recognizes the importance of full access to health care, and has moved aggressively to investigate and resolve such complaints. The Department has carefully studied the medical evidence about HIV and heeded the guidelines issued by the Centers for Disease Control governing safe treatment.63 The Department is also guided by the Supreme Court's decision in Bragdon v. Abbott,64 a case involving a dentist who refused to provide even the most routine dental care to a patient with HIV. The Court held that a medical provider may not refuse to treat by invoking the "direct threat" defense unless the risk of HIV transmission is "significant" and based on objective evidence.65
In 2003, the Department resolved allegations in a complaint filed by a young man who went to the Burleson St. Joseph Health Center in Burton, Texas, for treatment of sinusitis. In the course of providing his medical history, he disclosed that he had HIV. Several weeks later, the Health Center sent him a letter by certified mail informing him that he could no longer receive treatment at the clinic "due to [his] medical condition being out of the scope of service of our nurse practitioner," and suggesting that he see a physician in a town an hour away. Under the settlement agreement negotiated by the Department, Burleson St. Joseph agreed that it would no longer turn away patients with HIV whom it is otherwise qualified to treat, and employees would be trained about the nondiscrimination requirements of the ADA.66
Mark Bourdon alleged a similar experience when his doctor informed him that he would not treat him because of Mr. Bourdon's HIV. In May 2000, Mr. Bourdon consulted the Arizona Bone & Joint Specialists, Ltd., a sports medicine practice with offices in Phoenix and Scottsdale, about a strained muscle in his shoulder. At his initial visit, Mr. Bourdon disclosed he had HIV. When physical therapy failed to correct the problem, he asked his doctor about surgical options. Mr. Bourdon alleged that his doctor refused to perform surgery because of his HIV. Mr. Bourdon filed a lawsuit against his physician, and the Department intervened in 2003. The case settled prior to trial through a consent decree, in which Arizona Bone & Joint Specialists agreed to pay $120,000 in compensatory damages to Mr. Bourdon and $20,000 in civil penalties.67 The doctors adopted a nondiscrimination policy, and agreed in the future not to deny services to individuals with HIV or other disabilities.
Complaints are not limited to refusals to provide care in an office setting. The Department has also focused on the denial of care in an emergency situation. In 2001, John Gill Smith of Philadelphia called 9-1-1 because he believed he was having a heart attack. Paramedics employed by the City of Philadelphia arrived on the scene and, after being informed of Mr. Smith's HIV status, refused to provide the pre-hospital care that would have been reasonable and appropriate for an individual complaining of chest pains. Mr. Smith alleged that they refused to touch him or assess his condition and refused to give him physical assistance in getting out of his home and into the ambulance. He alleged that on the way to the hospital he was verbally harassed and insulted because of his HIV status. The Department filed suit in 2004 seeking to prevent the City's EMS providers from discriminating against individuals with HIV and seeking an award of compensatory damages for Mr. Smith.68 The parties are in settlement discussions to resolve issues in the case. If settlement fails, the case will be scheduled for trial.
C. Gateways to Job Opportunities for People with Disabilities
1. Employment
"Prejudice, we are beginning to understand, rises not from malice or hostile animus alone. It may result as well from insensitivity caused by simple want of careful, rational reflection or from some instinctive mechanism to guard against people who appear to be different in some respects from ourselves. Quite apart from any historical documentation, knowledge of our own human instincts teaches that persons who find it difficult to perform routine functions by reason of some mental or physical impairment might at first seem unsettling to us, unless we are guided by the better angels of our nature."
– Justice Anthony Kennedy69
As we move through the 21st century, a strong economy, the increasing need to replace large numbers of workers exiting the workforce through retirement, and the ready pool of qualified workers with disabilities present an historic opportunity to fulfill the promise of unlimited employment opportunities for people with disabilities. By the year 2014, 36 million people are expected to leave their jobs and will need to be replaced.70 Fully ten percent of undergraduate students – that is, over 1.5 million individuals – report having one or more disabilities.71 It is more important than ever to ensure that people with disabilities in the workforce, and those seeking to enter it, are not turned aside by discrimination.
Responsibility for eliminating disability-based employment discrimination is shared by the Department of Justice and the Equal Employment Opportunity Commission ("EEOC"). The EEOC is responsible for ensuring nondiscrimination in private sector employment and the Department is responsible for ensuring nondiscrimination in employment by state and local government employers. In United States v. Tennessee, the Department challenged Tennessee's blanket statutory exclusion of all individuals with "apparent mental disorders" from employment as sheriffs, police officers, correctional officers, and youth service officers. The case came to the Department's attention after two 9-1-1 dispatchers employed by Weakley County were suddenly subjected to psychological evaluations in 1997 and subsequently terminated even though they had successfully performed their jobs for several years. Under a 2003 consent decree with the Department, Tennessee agreed to stop enforcing the policies, to ask the legislature to rescind the statutes, and to draft new policies pursuent [sic] to the ADA.72
Some discrimination, as in Tennessee, results from sweeping policies. Other forms are more individualized, such as that faced by a Baltimore City public school teacher. In United States v. Baltimore Public Schools, an elementary school teacher who is blind applied for a teaching position with the Baltimore school system. During her two interviews, she used a cane. She was offered a job. When she mentioned that she would soon be picking up her new service animal, the school principal withdrew the job offer. In its 2001 consent decree with the Department, Baltimore agreed to pay the teacher $55,000 in damages and appointed an ADA coordinator for employment matters to help prevent future discrimination.73
In Missouri, a nurses' aid, whose job duties consisted of bathing, grooming, feeding, and generally caring for elderly patients in a nursing home, disclosed to her employer that she had contracted HIV. She alleged that even though her job did not include any invasive procedures, she was promptly terminated because of her disability. In its 2006 consent decree with the Department, Marion County Nursing Home agreed to pay the assistant $25,000 in damages, and agreed to change its employment policies to conform to the requirements of the ADA.74
After many years of hard work, Ronnie Collins entered the police academy to begin training as a state highway patrol trooper. While attending the rigorous, military-style cadet training academy, he asked for additional food as a reasonable accommodation for his diabetes. When it was denied, his blood sugar allegedly became dangerously low, and, as a result, he became combative and was unable to timely report for training. He was then terminated from the academy, rendering him unable to work as a trooper. In its 2004 consent decree with the Department, the Mississippi Department of Public Safety agreed to pay Mr. Collins $35,000 in damages, adopt and institute a reasonable accommodation policy, and train academy personnel about diabetes.75
"It was important to me to know that because of the ADA, the discrimination I encountered because of my diabetes was unlawful and would not happen to others."
- E-mail dated August 12, 2006, from Ronnie Collins
In each of these cases, qualified individuals were denied employment opportunities in a variety of necessary and important jobs simply because they had, or were perceived as having, a disability. The ADA was designed to address situations such as these. Enforcement of the ADA through education, mediation, and litigation is designed to ensure that employers hire and retain individuals with disabilities, and those that are perceived to be disabled, based on merit alone.
Title I of the Americans with Disabilities Act of 1990 prohibits private employers, state and local governments, employment agencies, and labor unions from discriminating against qualified individuals with disabilities in job application procedures, hiring, firing, advancement, compensation, job training, and other terms, conditions, and privileges of employment. The ADA covers employers with 15 or more employees. The ADA’s nondiscrimination standards also apply to federal sector employees under Section 501 of the Rehabilitation Act, as amended, and its implementing rules.
2. Higher Education
As more students with disabilities acquire high school degrees, an increasing number are seeking the opportunities presented by higher education – at two-year colleges or trade schools, universities, and graduate schools. But many students with disabilities face barriers to full enjoyment of their educational experience. These barriers to education in turn make it much more difficult for people with disabilities to achieve their full potential in the labor market.
For example, a student with a mobility impairment may be limited to courses offered in buildings and classrooms that are accessible. And even where she can enter a classroom building, she may not be able to use the laboratory equipment in a science class, open the door to an English classroom, pull up in her wheelchair to the stations in a computer science class, find seating in a history lecture, or visit her professor's office. She may have to go to another building to use an accessible restroom or water fountain. But the route to that building may be blocked by construction debris or may not have curb cuts that enable her to cross the street. There may be no signs to direct her to an accessible entrance to a facility.
Her classmate who is hard of hearing may not be provided an assistive listening device in an auditorium so that he can understand the instructor's words. If fire alarms or emergency announcements in his residence hall or the library do not include a visual component, he will not be aware of them.
A student with a vision impairment may be lost on campus without the benefit of signs that have Braille or raised lettering, and that designate names of rooms or indicate directions to certain locations. She can be harmed by protruding objects – like temporary or permanent hanging signs or certain water fountains – if they are placed in a location that her cane cannot detect.
The Department has been vigilant in responding to complaints of barriers to education. In one 2002 case, the Department investigated a complaint that a number of buildings and facilities on the campus of Millikin University in Illinois were not accessible to people with mobility impairments. Students with mobility impairments allegedly could not access some of the residential facilities offered by the University and could not go from one level of the student union to another without exiting the building. Under a settlement agreement with the Department, the University made a broad range of its campus activities accessible to people with disabilities.76 It agreed to modify entrances, counters, food service lines, telephones, bathrooms, drinking fountains, dining booths, doors, tables, and picnic areas; to repair sidewalks and curbs in order to create accessible routes between buildings; to install an elevator in the student union; and to provide accessible wheelchair seating locations and assistive listening devices in lecture halls.
In 2005, the Department began an initiative to review a number of private colleges and universities, including proprietary schools, in various parts of the country, even absent a specific complaint. The Department recently announced its first two comprehensive agreements with the University of Chicago and Colorado College,77 with others anticipated soon. Both agreements address a wide array of issues and require the schools to ensure increased access to their campuses for students, faculty, and visitors – in particular those with mobility, hearing, and vision impairments. For example, the colleges will:
-
submit accessibility plans outlining proposals to comply with the agreement to the Department for review after seeking public comment;
-
implement campus-wide emergency evacuation, sheltering, and shelter-in-place plans for individuals with disabilities after public comment and Department review;
-
ensure that three percent of the units (and adjacent toilet rooms) in student living facilities are accessible and dispersed among the facilities, and that a reasonable number of housing facilities have an accessible entrance, first floor common area, and toilet room that is usable by a visitor with a disability;
-
display information on their websites identifying accessible routes through the campuses, accessible parking areas, accessible entrances to buildings, and accessible spaces within buildings;
-
post signs at facility entrances and toilet rooms identifying those that are accessible and, at inaccessible entrances and toilet rooms, directing individuals to the nearest accessible entrance or toilet room;
-
provide assistive listening devices for people with hearing impairments in lecture halls, meeting rooms, auditoria, and other assembly areas;
-
move classes and other activities to fully accessible locations when necessary; and
-
correct violations of the accessibility standards for new construction.
The University of Chicago also agreed to ensure that its transportation services – including its fixed-route campus-wide bus system and its on-call evening and night-time service – satisfy the requirements of the ADA.

The University of Chicago's Old Quad.

The University of Chicago's Palevsky Dormitory.
More and more students, including those with disabilities, are also continuing their education by attending graduate school or postgraduate professional school. But some students with disabilities face discrimination in taking the admissions tests or the classes that prepare students for those tests. In 2002, the Department filed suit against the Law School Admission Council, the agency that administers the Law School Admission Test, based on complaints that the Council had failed to provide reasonable testing accommodations to four persons with disabilities. The individuals had requested extra time to complete the examination because of their physical disability, cerebral palsy. But the Council inappropriately insisted that the applicants undergo testing for learning disabilities, without which they would not be granted extra time. Under the terms of the consent decree resolving the case, the Council agreed to grant the requested testing accommodation to candidates who have been granted the same or comparable accommodation on other standardized admission tests; give considerable weight to the recommendation of the candidate's doctor or other evaluator; not require individuals to undergo diagnostic or functional tests that are unnecessary or not commonly utilized by the medical community; and pay $20,000 in damages.78
In June 2006, the Department filed suit against and reached a consent order with TestMasters, one of the nation's largest providers of preparatory courses for graduate school admissions tests.79 This action was based on a complaint by a deaf individual, who was denied a sign language interpreter for a class preparing for the Law School Admission Test. When he complained to the company that they were violating the ADA, the company canceled his registration and would not allow him to take the class. Under the consent order, TestMasters agreed to provide auxiliary aids to students who need them for its preparatory courses nationwide. TestMasters also agreed to appoint an ADA coordinator, train its staff regarding the company's obligations under the ADA, pay $20,000 in damages to the deaf student, and pay $10,000 in civil penalties.
3. Childcare
"I work 40 hours a week on the southwest side of town. This act alone [refusing to provide care for my child] brought me to tears. Having to make such an important decision, I was left with no other choice than to inform my employer that I could not return back to work until I successfully found adequate child care for my son."
- Complaint received by Disability Rights Section in 2005
The Department of Justice receives a large number of complaints that echo this story. The Department is committed to rooting out discrimination against children with disabilities, in part because of the importance of giving parents of children with disabilities the opportunity to participate in the workforce. Recent Census Bureau data shows that two percent of children under the age of three and 3.6 percent of children between the ages of three and five have some type of disability.80 The U.S. Department of Labor's Bureau of Labor Statistics recently reported that nearly 63 percent of the nation's children under the age of five have mothers in the workforce and require some childcare arrangement.81 Fifty-three percent of school-aged children between the ages of five and fourteen also require some type of weekly childcare arrangement, including access to summer camps and after-school care.82
Childcare providers that meet the definition of public accommodation – essentially those childcare providers that provide services open to the public, but not including childcare operated by religious organizations or entities controlled by religious organizations – regardless of size or number of employees, must comply with Title III of the ADA. Similarly, Title II of the ADA applies to childcare centers run by public entities, including Headstart programs and other state and local programs that provide childcare. The ADA prohibits childcare providers from discriminating against persons with disabilities on the basis of disability. Under federal regulations, childcare providers must allow children and parents with disabilities an equal opportunity to participate in the childcare center's programs and services. Specifically, the ADA and/or its regulations provide that:
-
Covered centers cannot exclude children with disabilities from admission to, or integration within, their programs unless their presence would pose a significant risk to the health or safety of others, would require a fundamental alteration of the program, or would result in an undue burden to the center.
-
Covered centers must provide appropriate auxiliary aids and services needed for effective communication with children or adults with disabilities, unless doing so would constitute an undue burden or would fundamentally alter the program.
-
Covered centers must generally make their facilities accessible to persons with disabilities. Existing facilities are subject to the readily achievable standard for barrier removal, while newly constructed facilities and any altered portions of existing facilities must be fully accessible.
"After around a week, [the childcare provider] finally called me back. She said she had discussed [my child's] case with her supervisor, the school nurse, and the school's attorney and informed me that they would be unable to accept our application. . . . I tried to explain that there's no reason to treat a child with a shunt any differently much less exclude him. Many people with vp shunts lead normal lives – I don't think you guys really understand the situation, what a shunt is and what needs to be done or even what can be done to deal with it. She said she understood, but kids [my son's] age fall all the time so it will be difficult to prevent that. . . I explained again that nobody can prevent kids from falling, we just try to do our best. . . . But I never imagined it could lead to his exclusion and I'm still astounded that [the facility] would discriminate against anyone with this condition. And the horrifying thing is the implication that other schools, clubs, etc. might treat [our child] the same way in the future. Then where can he go? How can he have a normal life?. . . The goal of filing this complaint is. . . to know that our son can't and won't be discriminated against as he goes through life."
- Complaint received by Disability Rights Section in 2005
The ADA is designed to ensure that decisions affecting persons with disabilities are based on the reality of each individual's situation. This is frequently not the case in childcare settings. Some childcare providers wrongly assume that a child's disabilities are too severe for the child to be integrated successfully into the center's childcare program. Federal regulations require a childcare provider to make an individualized assessment about whether it can appropriately meet the particular needs of a child within its program. Providers are often surprised at how simple it is to include children with disabilities in their mainstream programs.
For example, in 2004 the Department settled a complaint against the Rieck Avenue Country Day School, alleging that the privately-owned childcare facility in Millville, New Jersey, had refused to enroll a seven-year-old girl with cerebral palsy and epilepsy in a summer program.83 According to the complaint, the girl's mother called the owner-director of the facility to inquire about openings in its summer program. The daughter had just finished first grade and had been attending public school and daycare since the age of eighteen months. She required no additional assistance with daily care or age-appropriate activities, and no modifications to the center's activities or programs were anticipated, with one exception: staff members would need to be informed that she had occasional petit mal seizures, after which she would be very tired or fall asleep. Under the agreement, the facility agreed to adopt a nondiscrimination policy and to publicize that policy in its handbooks for parents and employees. The facility also agreed to provide training to management and staff about the obligations of childcare providers concerning the rights of individuals with disabilities. Lastly, it agreed to pay the mother, on behalf of her daughter, $4000 in compensatory damages.
Sometimes, problems may be solved by childcare providers simply permitting more flexibility in their rules and policies. For example, in 2003 the Department resolved a matter against a Texas childcare center that allegedly refused to enroll a four-year-old child with Down Syndrome who needed diapering.84 The center had a policy of requiring children over the age of three to be toilet trained. The provider agreed to pay $4000 in damages to the complainants, modify its policy to admit children over three who are not toilet-trained if their need for diapering is due to a disability, and provide ADA training to its employees.
"My two year old son was recently barred from enrolling in a day care center because 'they can't handle another special needs child.'. . . he has a diagnosis on the autism spectrum, widely considered by everyone who has seen him to be mild and very treatable. He does not have autism, and he functions well in a typical day care setting and has since he was three months old. . . . I have carefully reviewed Title III of the ADA. A day care center cannot refuse a child on the basis of disability unless he is a physical danger or admitting him would fundamentally change the nature of the program. Neither are true. . . .I would ask you to let them know that they cannot discriminate against children who are not completely typical. I never expected to have my son discriminated against so early in his life."
- Complaint received by Disability Rights Section in 2005.
All children in childcare settings require a certain amount of daily individualized attention. The Department has received complaints alleging that childcare providers are refusing to extend their services to children with disabilities, claiming that they are unable to adequately serve the children. In many instances, the child with disabilities needs little, if any, modification to the program to successfully participate. For children with more severe impairments, modifications can often be made that do not fundamentally alter the provider's programs.
If a child does, however, need one-on-one attention due to a disability, it is still possible that, in certain circumstances, the child can be integrated into a childcare program with reasonable modifications that do not fundamentally alter the program. For instance, consider a child with Down Syndrome and significant mental retardation who applies for admission to a childcare program but who needs one-on-one care to benefit fully from the childcare program. If a personal assistant will be provided at no cost to the childcare center (usually by the parents or through a government program), the child can likely be integrated with reasonable modifications to allow for the child's one-on-one care within the program. (This is not to suggest that all children with Down Syndrome need one-on-one care or must be accompanied by a personal assistant in order to be successfully integrated into a mainstream childcare program.) It is important to note that the ADA generally does not require centers to hire additional staff or provide constant one-on-one supervision of a particular child with a disability.
The Department also has provided technical assistance to centers to enable the providers to find ways to accommodate children with severe allergies. For example, in 2006, the Department offered technical assistance to a large language immersion summer camp program in the Midwest that had refused to enroll a child with severe food allergies because the provider would not agree to administer epinephrine via an "Epi-pen Junior" in the event of a life-threatening emergency. After receiving technical assistance from the Department, the camp decided to enroll the child and she participated successfully in the camp program.
Similarly, the Department has helped children with diabetes, who can usually be integrated into a program without fundamentally altering it, to participate in various children's programs.
"We are very grateful to the Department of Justice for their interest in Eleanor's case [against TSI] and for their efforts on behalf of her and all diabetic children."
- E-mail dated August 8, 2006 from Quint Medley and Kay Thompson, parents of Eleanor
For example, in 2006 the Department entered into a consent decree with Town Sports International, Inc., and its Wellesley, Massachusetts camp to resolve a lawsuit filed by parents of a child with insulin-dependant diabetes and to ensure equal opportunity for children with diabetes at Town Sports camps and programs.85 The consent decree, filed in the United States District Court in Boston, resolved allegations that Town Sports excluded the elementary school student because of both her diabetes and her use of an insulin pump to control her diabetes in violation of the ADA. The company and its local sport club have agreed to evaluate the application of each child with diabetes who applies to any Town Sports International camp in the United States on a case-by-case basis and to make reasonable modifications to permit children with diabetes to attend its camps. TSI agreed to supervise campers while the campers check their blood glucose levels and use insulin pumps, syringes, or other diabetes-related medical equipment, and to monitor the campers' consumption of food. The consent decree also required Town Sports International to pay $25,000 in damages to the plaintiff and $5000 in civil penalties.
Kay Thompson and daughter Eleanor.
Finally, the Department continues to work to eliminate discrimination against children without disabilities who face discrimination because of the disability status of their parents. The Department reached an agreement with Wee-Kare Nursery, a home-based daycare center in Virginia, resolving a complaint that the childcare provider had terminated a child from its program because his mother had hepatitis C.86 Allegedly, after the child's mother told the daycare owner in confidence that the reason she had been going to so many doctor's appointments was because of her hepatitis C, the nursery owner said that she would no longer take care of her son, even though the child had tested negative for hepatitis C. The owner of the facility also allegedly told the parents of other children in the program of the parent's health issues. The owner agreed to attend a training program on the ADA obligations of childcare providers, adopt a written nondiscrimination policy, and pay $1000 in compensatory damages to the complainant.
D. Enjoying the American Way of Life
1. Entertainment and Leisure
Recreational activities for children and adults, ranging from bowling and water aerobics to softball, baseball, basketball, and soccer leagues, play a critical role in the lives of many Americans. Recreation vastly improves the quality of people's daily lives. Unfortunately, many adults and children with disabilities have been excluded from participating in many games and activities not by choice, but by exclusionary policies that put them on the sidelines.
The ADA addresses this problem by giving people with disabilities an equal opportunity to participate in most recreational activities unless participation by a person with a disability would pose an undue burden or would fundamentally alter the recreational activity. The United States Supreme Court endorsed this concept of equal participation for people with disabilities when it held in PGA Tour, Inc. v. Martin that it was appropriate to reasonably modify a rule banning golf carts when necessary to allow a disabled professional golfer to participate.87
The Department has worked to advance this important goal for people with disabilities. For example, a deaf referee in the Eastern College Athletic Conference (ECAC) alleged that her officiating assignments were reduced and she was excused from the otherwise mandatory referee camp for women's basketball officials because she required a sign language interpreter. The Department entered into a 2003 settlement agreement with the ECAC to provide her with an equal opportunity to officiate at games, to provide appropriate auxiliary aids and services, and to notify its member institutions about the ADA's requirement for effective communication.88
- E-mail dated August 17, 2006, from Justin "Pono" Tokioka, age 11.
The Department and PONY Baseball, Inc. signed a 2006 settlement agreement that will ensure that players who are disabled, including those who are deaf or hard of hearing, have an equal opportunity to participate in PONY's 3500 baseball and softball leagues.89 The agreement stemmed from a complaint from the parents of Justin "Pono" Tokioka, who alleged that their son was denied access to a sign language interpreter during a 2005 PONY baseball tournament. As part of the settlement agreement, PONY agreed to modify its rules to allow players to use sign language interpreters during games, provide sign language interpreters for players who are deaf or hard of hearing, and make reasonable modifications to its rules and practices to allow players with disabilities an equal opportunity to participate.
These examples illustrate how simple modifications in policies or reasonable accommodations can have a profound impact on individuals with disabilities – and can make the difference between enjoyment and exclusion.
During the congressional hearings preceding the passage of the ADA, reports, surveys, and testimony offered by numerous witnesses made plain that many persons with disabilities led isolated lives and did not frequent places of public accommodation. For example, according to one national poll: "The survey results dealing with social life and leisure experiences paint a sobering picture of an isolated and secluded population of individuals with disabilities. The large majority of people with disabilities do not go to movies, do not go to the theater, do not go to see musical performances, and do not go to sports events."90 To address these problems, Title III of the ADA expressly prohibits disability-based discrimination at places of public accommodation and commercial facilities, including movie theaters, sports arenas, concert halls, and outdoor stadiums. Over the last five years, the Department has made great strides toward ensuring that persons with disabilities, along with their families and friends, have equal access to, and full enjoyment of, popular entertainment venues on the same terms as other Americans.
When trying to attend entertainment events at places of public accommodation, people with disabilities frequently face discrimination in ticketing policies and practices. Such problems range from unequal ticketing services to inaccessible ticket counters and the unavailability of accessible seating in stadiums, concert halls, theaters, or sports facilities. Over the last several years, the Department has focused its enforcement efforts on correcting these inequities. For example, in 2002 the Department signed settlement agreements with a number of theaters in Branson, Missouri, which, among other things, required the theaters to provide accessible ticket counters and to implement new ticketing policies so that designated accessible seating is held for customers with disabilities until all other seating has been filled.91
The Department also signed a wide-ranging settlement agreement in 2005 with the world's largest ticketing company – Ticketmaster, Inc. – requiring it to make its ticketing services more accessible to persons with disabilities.92 In this agreement, Ticketmaster agreed to make agents available to sell accessible seating via telephone and e-mail during all hours its system is operational. Ticketmaster also agreed to take appropriate steps to inform customers promptly if its inventory of accessible seating is sold out and whether additional seating might be available directly from the venue. In addition, Ticketmaster will work with venues to implement procedures to reserve the inventory of unsold accessible seats for customers with disabilities until two weeks prior to the event, even if general seating is sold out, and will continue its efforts to develop a system to sell accessible seating directly on its website.
Another hurdle commonly faced by persons with disabilities and their companions when at-tending entertainment events at public facilities is inferior and uncomfortable seating locations. The Department's ADA regulations require public accommodations to provide persons with disabilities choices of admission prices and lines of sight comparable to other members of the audience. All too often, however, persons with disabilities and their companions are offered few – if any – seating choices and instead are relegated to the least desirable seating locations with painful or distorted views of the stage or screen. These problems have proven particularly acute at most of the existing stadium-style movie theaters around the country in which persons with disabilities are often compelled to sit outside the stadium section in the rows closest to the screen. One disabled veteran described his seating location near the front of one stadium-style theater as follows:
"[S]omewhere where before I was in a [wheel]chair I wouldn't even dream of sitting because of the location. A lot of times it's where the parents put their kids, and they sit in better rows. So there's a lot of commotion in that area down front. I have been kicked in the head by a kid flipping over in the seats, all that, so that's why I call it the pit area . . . . You are looking more up. And my chair doesn't recline like your movie chairs. You sit in this position and you can recline somewhat, and my chair doesn't. So I'm . . . watching a movie and always trying to get the full screen effect, and it bothers your neck, my back and sometimes you get headaches . . . . I go out of the theater, out to their lobby area, and my wife helps me. . .stretch around. And then after about five minutes or whatever, we go back in . . . . I would like to be able to – you know, I pay the money, the same price everyone else pays. I would like to be able to be comfortable, sit through the movie with my family or wife and see the movie, you know, the way I used to be able to. Now I am restricted to where they want me to sit. So I have no options.93

A typical stadium-style movie theater
To address such inequities, the Department has reached nationwide settlements with, or had court orders entered against, the largest theater chains in the country – including the Regal Entertainment Group, Cinemark USA, Inc., National Amusements, Inc., Hoyts Cinemas Corporation, and AMC Entertainment, Inc. Under a consent decree entered in United States v. Cinemark,94 that chain must design new theaters in accordance with Department guidance and approval, placing wheelchair locations in the middle of each auditorium. Cinemark agreed to move wheelchair locations back in over 100 theaters within the jurisdiction of the Sixth Circuit (which covers Tennessee, Kentucky, Ohio, and Michigan) and at theaters in California, Illinois, New York, Utah, and Oregon. The United States negotiated a nationwide consent decree in United States v. Regal Entertainment Group as well, delivering improved sight lines for persons who use wheelchairs across the largest movie theater chain in the country, covering over 3,500 screens.95 Regal agreed to provide improved lines of sight in both existing and new construction movie auditoriums. All future construction will place wheelchair locations in the middle of the seating area, where other patrons choose to sit. A consent order was entered in United States v. National Amusements that provides similar relief at the National Amusements chain.96 Each of these agreements or court orders requires the respective movie theater company to construct ramps to the stadium section in specified auditoriums in their respective stadium-style theaters; to move wheelchair and companion seating farther back from the screen in additional auditoriums; and to correct other ADA violations (such as non-compliant companion seating) as necessary in other auditoriums. These agreements and orders include design standards for stadium-style theaters to be constructed that mirror the Department's proposed regulatory standards set forth in the Department's Advanced Notice of Proposed Rulemaking issued in September 2004.97 Further, in the AMC litigation, the Court ordered AMC to pay civil penalties of $100,000 and compensatory damages to patrons with disabilities who had suffered discrimination.
The Department's enforcement efforts with respect to addressing seating issues in public accommodations has also included other entertainment venues, such as concert halls and opera houses. The Department entered into a Consent Decree in 2005 with the Apollo Theater Foundation, which operates the historic Apollo Theater in Harlem, requiring the theater to install twelve permanent wheelchair seating locations with companion seats in its orchestra section, as well as to correct other barriers to access at the theater.98 In addition, the Department entered a Consent Decree in 2003 with the Shubert Organization, Inc., to make live theater venues in New York City, both on and off Broadway, more accessible. Wheelchair seating was added in sixteen theaters and ticketing practices have been improved so that tickets for wheelchair seating will be held for persons with disabilities until all other seating is sold out. Shubert also paid civil penalties of $50,000. And, in 2004 the Department settled with the City of Des Moines, requiring the city to make the outdoor riverside Simon Estes Amphitheater more accessible to persons with disabilities by installing a lift and ramps to provide access to newly designated wheelchair seating areas and by installing an assistive listening system for persons who are deaf or hard of hearing.99
Wheelchair users can now enjoy the historic Apollo Theater in Harlem.
In another agreement, the Washington Opera Company in Washington, D.C., agreed in 2002 to increase the number and locations of accessible seats at its performances held offsite while the Opera House at the John F. Kennedy Center for the Performing Arts was undergoing renovation.100 These new accessible seating locations were dispersed throughout the orchestra section and sold at all of the price categories offered to the general public. In addition, Washington Opera agreed to designate an ADA coordinator, create an ADA advisory committee, and conduct extensive advertising about the availability, pricing, and locations of accessible seating. Structural improvements at the Kennedy Center Opera House also led to more accessible seating at Washington Opera performances. These improvements included increasing the amount of accessible seating dispersed throughout the renovated auditorium. Previously, the only wheelchair-accessible seats in the Kennedy Center Opera House were the most expensive seats.
A ramp and accessible seating at the Huntsville Speedway in Huntsville, Alabama
Now, opera fans at these facilities who use wheelchairs truly have an equal opportunity to enjoy performances as they enjoy admission price choices and lines of sight comparable to those afforded the general public.
In addition to seating problems, persons with disabilities frequently encounter inaccessible lobbies, concession counters, restrooms, parking lots, or other architectural features outside the seating areas of places of public accommodations. Settlement agreements and consent decrees over the last five years have also led to significant corrections in such inaccessible features outside the seating areas at a wide variety of establishments – including AMC stadium-style movie theaters nationwide; the Apollo Theater in New York, New York; the White House Theater, Mel Tillis Theater, and Magical Palace in Branson, Missouri; the Huntsville Speedway in Huntsville, Alabama;101 the M&T Bank Stadium (formerly known as PSINet Stadium) in Baltimore, Maryland;102 the West Orange YMCA in Orlando, Florida;103 and the Brookside Gardens near Washington, D.C.104 In the Huntsville Speedway case, for example, the owner has agreed to make physical modifications to ticket counters and toilet rooms for spectators and racers, to improve spectator seating, and to increase accessible routes to the seating.
One final area addressed by the Department concerns the ability of persons with disabilities to safely enjoy entertainment events at places of public accommodation without fear of discriminatory rules restricting access to prescription drugs or other necessary medical supplies.

Jim Radermacher and family.
- E-mail dated July 31, 2006, from Jim Radermacher, complainant in United States v. SFX Entertainment, Inc.
In 2003, Clear Channel Entertainment settled with the Department to resolve a lawsuit challenging Clear Channel's policy of prohibiting individuals with diabetes from keeping their medical supplies with them while attending concerts in the 100-plus concert venues owned or operated by Clear Channel throughout the country.105 The policy prohibited patrons from taking any syringes or needles used for medical purposes, including needles used for insulin and lancets for testing blood, into the concert venue unless secured in a first aid room. The policy allegedly violated Title III of the ADA by denying individuals with diabetes an equal opportunity to attend and enjoy concerts since many individuals with diabetes who use insulin must test their blood sugar with lancets and inject insulin with syringes. Lack of immediate access to blood testing equipment, food and/or glucose, and insulin can be life-threatening for such individuals. Under the consent decree, Clear Channel agreed to adopt a new policy that allows individuals with diabetes to keep their medical supplies with them at concerts, to pay damages to the complainants, and to train its employees on its new policy.
"When I was separated from a concert line for carrying my diabetic supplies I was incredibly embarrassed. I felt as if I was being treated like a criminal. My embarrassment quickly turned to anger ... I needed to keep my supplies with me in order to maintain safe controls of my blood sugars. I honestly did not want any other diabetic to experience the humiliation I felt ... the ADA was so quick to respond and so genuinely concerned...I had a renewed strength in keeping my medical needs and health a priority. I will always be grateful to the ADA."
- E-mail dated August 5, 2006, from Mary Jungenberg, complainant in United States v. SFX Entertainment, Inc.

Mary Jungenberg
Footnotes
37 28 C.F.R. pt. 36 app. A (2005).
38 See, e.g., Settlement Agreements entered into by the United States with the following communities: Omaha, Neb. (July 25, 2005), available at http://www.ada.gov/omahanesa.htm; Suffolk, Va. (Sept. 27, 2004), available at http://www.ada.gov/suffolkva.htm; Pueblo, Colo. (June 2, 2004), available at http://www.ada.gov/pueblo.htm; Juneau, Alaska (Aug. 5, 2004), available at http://www.ada.gov/JuneauSA.htm; Gallup, N.M. (Sept. 24, 2004), available at http://www.ada.gov/gallupnm.htm; and San Luis Obispo, Cal. (Dec. 14, 2004), available at http://www.ada.gov/sanluis.htm.
39 Press Release, U.S. Dep't of Justice, Justice Department to Meet with San Antonio Officials as Part of Initiative to Ensure Civic Access for People With Disabilities (July 24, 2002), available at http://www.ada.gov/sanapr.htm.
40 U.S. Dep't of Justice, ADA Stories - San Antonio, Texas, available at http://www.ada.gov/sanastor.htm.
41 Press Release, U.S. Dep't of Justice, Justice Department to Meet with Springfield Officials as Part of Initiative to Ensure Civic Access for People With Disabilities (July 24, 2002), available at http://www.ada.gov/sprstpr.htm.
42 U.S. Dep't of Justice, ADA Stories - Springfield, Missouri, available at http://www.ada.gov/sprstor.htm.
43 Id.
44 Settlement Agreement between the United States and the City of Juneau, Alaska (Aug. 5, 2004), available at http://www.ada.gov/JuneauSA.htm.
45 Settlement Agreement between the United States and Florence County, S.C. (May 5, 2005), available at http://www.ada. gov/florencesc.htm.
46 Settlement Agreement between the United States and Arlington County, Va. (Mar. 30, 2006), available at http://www.ada. gov/arlingsa.htm.
47 Settlement Agreement between the United States and the Staten Island Univ. Hosp. (Aug. 6, 2003).
48 United States v. Parkway Hosp., Inc., No. 03-1565 (E.D.N.Y. Apr. 29, 2004), available at http://www.ada.gov/parkway.htm.
49 Gillespie v. Dimensions Health Corp., d/b/a Laurel Reg. Hosp., No. 05-73 (D. Md.), available at http://www.ada.gov/laurelco.htm.
50 See, e.g., Parkway Hosp., supra n. 48 (allegations included inappropriate reliance on adult hearing daughter for all communications between hospital and deaf patient and spouse).
51 Gillespie and United States v. Dimension Health Corp. d/b/a Laurel Reg. Hosp., No. 05-73 (D. Md. July 12, 2006), available at http://www.ada.gov/laurelco.htm.
52 See, e.g., Parkway Hosp., supra n. 48; Settlement Agreement between the United States and Advocate Ravenswood Hosp. Med. Ctr. (Apr. 3, 2001).
53 United States v. Fairview Health Serv., No. 04-4955 (D. Minn. Dec. 8, 2004), available at http://www.ada.gov/fairview.htm.
54 See Settlement Agreements entered into by the United States with Greater Southeast Cmty. Hosp. (June 22, 2005), available at http://www.ada.gov/secommhosp.htm; St. Francis Healthcare (Nov. 4, 2005); and South Florida Baptist Hosp. (May 5, 2006).
55 United States v. Saimovici, No. 05-7712 (S.D.N.Y. Sept. 1, 2005).
56 Settlement Agreement between the United States and Dr. Ray Hand (Aug. 17, 2005), available at http://www.ada.gov/ rhandsa.htm.
57 Settlement Agreement between the United States and Modern Dental Professional, Indiana, P.C. (Apr. 17, 2006).
58 Settlement Agreement between the United States and Exodus Women's Center (Apr. 26, 2005), available at http://www.ada.gov/exodus.htm.
59 Settlement Agreement between the United States and Georgetown Univ. Hosp. (Oct. 31, 2001), available at http://www.ada.gov/gtownhos.htm.
60 Settlement Agreement between the United States and Dr. Robila Ashfaq (Jan. 12, 2005), available at http://www.ada.gov/drashfaq.htm.
61 Settlement Agreement between the United States and Washington Hosp. Ctr. (Nov. 2, 2005), available at http://www.ada. gov/ whc.htm.
62 Settlement Agreement between the United States and Valley Radiologists Med. Group (Nov. 2, 2005), available at http://www.ada.gov/vri.htm.
63 See, e.g., Centers for Disease Control, Recommendations for Preventing Transmission of Human Immunodeficiency Virus and Hepatitis B During Exposure-Prone Invasive Procedures, Morbidity and Mortality Weekly Report (July 12, 1991), Vol. 40, (RR08), 1-9; Guidelines for Prevention of Transmission of Human Immunodeficiency Virus and Hepatitis B Virus to Health-Care and Public-Safety Workers, Morbidity and Mortality Weekly Report (June 23, 1989), Vol. 38, No. S-6; Recommendations for Prevention of HIV Transmission in Health-Care Settings, Morbidity and Mortality Weekly Report (Aug. 21, 1987), Vol. 36, No. 2S.
64 Bragdon v. Abbott, 524 U.S. 625 (1998).
65 Id. at 649-55.
66 Settlement Agreement between the United States and the Burleson St. Joseph Health Ctr. (Apr. 21, 2003).
67 Bourdon and United States v. Croft, No. 02-1233 (D. Ariz. Feb. 10, 2004), available at http://www.ada.gov/bourdoncons.htm.
68 Smith and United States v. City of Philadelphia, No. 03-6494 (E.D. Pa. 2004).
69 Board of Trustees of the University of Alabama v. Garrett, 531 U.S. 356, 374 (2001) (Kennedy, J., concurring).
70 W. Roy Grizzard, Ed.D., Assistant Sec'y of Labor, Luncheon Keynote Address, Diversity Profit Generation Series: Proving the Financial Business Case for Diversity, New York, New York (June 20, 2006), available at http://www.dol.gov/odep/media/speeches/diversitynyc.htm.
71 Id.
72 United States v. Tennessee, No. 98-1357 (W.D. Tenn. Apr. 15, 2003), available at http://www.ada.gov/tennesse.htm.
73 United States v. Baltimore Pub. Schs., No. 01-4187 (D. Md. Dec. 31, 2001).
74 United States v. Marion County Nursing Home, Inc., No. 05-70 (E.D. Mo. Feb. 2, 2006).
75 United States v. Mississippi Dep't of Pub. Safety, No. 00-377 (S.D. Miss. Mar. 4, 2004), available at http://www.ada.gov/mdps.htm.
76 Settlement Agreement between the United States and Millikin Univ. (Mar. 14, 2002), available at http://www.ada.gov/millikin.htm.
77 Settlement Agreement between the United States and Univ. of Chicago (July 17, 2006), available at http://www.ada.gov/ unichicagosa.htm; and Settlement Agreement between the United States and Colorado Coll. (Aug. 3, 2006).
78 United States v. Law Sch. Admission Council, No. 99-6209 (E.D. Pa. Feb. 26, 2002), available at http://www.ada.gov/lsac.htm.
79 United States v. Robin Singh Educ. Servs. ("TestMasters"), No. 06-3466 (C.D. Cal. June 21, 2006).
80 U.S. Census Bureau, Survey of Income and Program Participation, June-September 2002.
81 U.S. Dep't of Labor, Bureau of Labor Statistics, Women in the Workforce: A Databook, May 2005.
82 U.S. Census Bureau, Who's Minding the Kids? Child Care Arrangements: Winter 2002 (2005).
83 Settlement Agreement between the United States and Rieck Ave. Country Day Sch., (June 2, 2004), available at http://www. ada.gov/rieckave.htm.
84 Settlement Agreement between the United States and Peggy's Child Care, Inc. (July 31, 2003).
85 E.M. v. Town Sports Int'l, Inc., and TSI Wellesley, Inc., No. 05-10611 (D. Mass. Apr. 10, 2006), available at http://www.ada.gov/ tsi.htm.
86 Settlement Agreement between the United States and Joetta Roberts (Nov. 18, 2003). 87 PGA Tour, Inc. v. Martin, 532 U.S. 661 (2001).
88 Settlement Agreement between the United States and the Eastern Coll. Athletic Conference (Oct. 21, 2003).
89 Settlement Agreement between the United States and PONY Baseball, Inc. (Aug. 17, 2006).
90 H.R. Rep. No. 101-485, pt. 2 at 34 (1990) (summarizing 1986 Lewis Harris poll).
91 Settlement Agreement between the United States of America and Mel Tillis Theater (Aug. 1, 2002), available at http://www. ada.gov/meltilth.htm; Settlement Agreement between the United States and Magical Palace (Sept. 30, 2002), available at http://www.ada.gov/magicpal.htm.
92 Settlement Agreement between the United States and Ticketmaster, Inc. (Dec. 22, 2005), available at http://www.ada.gov/ticketmaster.htm.
93 Statement of Uncontroverted Facts and Conclusions of Law in Support of Plaintiff United States' Motion for Partial Summary Judgment Re: Line of Sight Remedies at 14, United States v. AMC Entertainment, Inc., et al., No. 99-1034 (C.D. Cal. Nov. 18, 2002).
94 United States v. Cinemark USA, Inc., No. 99-705 (N.D. Ohio Nov. 5, 2004), available at http://www.ada.gov/cinemark/ cinemark4main.htm.
95 United States v. Hoyts Cinemas Corporation, Regal Entertainment Group, and Regal Cinemas, Inc., No. 00-12567 (Mass. June 8, 2005), available at http://www.ada.gov/regal.htm.
96 United States v. National Amusements, Inc., No. 00-12568 (Mass. Jan. 9, 2006), available at http://www.ada.gov/national.htm.
97 69 Fed. Reg. 58,768 (Sept. 30, 2004).
98 United States v. Apollo Theater Foundation, No. 05-5988 (S.D.N.Y. June 28, 2005), available at http://www.ada.gov/apollomain.htm.
99 Settlement Agreement between the United States and the City of Des Moines, Iowa (Jan. 29. 2004).
100 Settlement Agreement between the United States and the Washington Opera (Sept. 18, 2002), available at http://www.ada. gov/washoper.htm.
101 Settlement Agreement between the United States and Huntsville Speedway (Jan. 19, 2006).
102 Settlement Agreement between the United States and Maryland Stadium Auth. (Dec. 14, 2001), available at http://www .ada.gov/mstadium.htm.
103 Settlement Agreement between the United States and West Orange YMCA (Nov. 21, 2003).
104 Settlement Agreement between the United States and the Maryland Nat'l Capital Parks and Planning Comm'n (Oct. 20, 2003), available at http://www.ada.gov/brooksidegard.htm.
105 United States v. SFX Entertainment, Inc., d/b/a Clear Channel Entertainment (E.D. Pa. June 11, 2003), available at http://www. ada.gov/sfxinc.htm.
User Comments/Questions
Add Comment/Question