Section 4.0 Findings
4.1 Wheeled Mobility Device Dimensions
Figure 1 and Table 2 show the standards from the four countries and the variables they include on wheeled mobility device sizes. Selected research findings are shown in Figures 2-8.
Figure 1
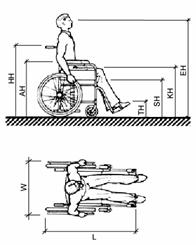
Table 2
|
|
U.S.* |
Australia |
Canada* |
U.K.* |
|
Unoccupied Width |
660 |
X |
660 |
X |
|
Unoccupied Length |
1065 |
X |
X |
X |
|
Handle Height (HH) |
915 |
X |
920 |
X |
|
Armrest Height (AH) |
760 |
X |
760 |
x |
|
Seat Height (SH) |
485 |
X |
480 |
480 |
|
Folded Wheelchair Width (F) |
X |
X |
300 |
X |
|
Occupied Width (W) |
X |
X |
X |
X |
|
Occupied Length (L) |
1200 |
X |
1200 |
X |
|
Eye Height (EH) |
1090-1295 |
1250 |
1100-1300 |
X |
|
Knee (Lap) Height (KH) |
685 |
X |
675 |
X |
|
Toe Height (TH) |
205 |
X |
200 |
X |
|
Toe Extension beyond Footrest (TE) |
150 |
X |
X |
X |
** Advisory information
Figure 2. Unoccupied Device Width
Figure 3. Unoccupied Device Length
The research data shows that the sizes of devices vary considerably from the values in the standards. The sizes described in the standards are close to the mean values found in the research studies but this is certainly not sufficient to accommodate a large enough proportion of wheeled mobility users. For example, the IDEA data for mean unoccupied length is identical to the standard. But, the widest device measured was about 150 mm wider and the longest more than 200 mm longer.
The data also indicates that armrest height and handle height vary considerably from the values included in standards but only for the extremes of the population (see figures 4-6). The means for these two variables were very close to the value in the standard in all three studies that measured it. In contrast, the mean seat height was above the value in the standard for the two studies that measured it and the difference between the value in the standards and the results is considerably larger than for armrest height and handle height.
Figures 4-5. Armrest Height
Figure 6. Handle Height
* One outlier removed due to data translation errors in software
The two studies that measured seat height discovered that the values in the current standards are below the means of the research results. This is probably due to the increased use of positioning systems, thick cushions and the availability of a wider range of wheel sizes since the 1970s but it can also be due to differences in measurement methods. The height of the seat can be measured at the edge and at the middle, under the cushion, or on top of the cushion. Thus, specifying exactly how it is measured is important for comparing results. In the IDEA research, the height of a seat plane was defined and also measured at point at the rear of an individual’s buttocks using an extension of the electromechanical probe that we slipped down behind an individual’s back. The results would clearly be different compared to other measurements, particularly if the measurement was taken at the leading or trailing edge of the seat below the cushion.
Figure 7. Seat Height
* Two outliers removed from IDEA Center data due to translation problems in software
For eye height, the findings are extremely consistent. They show that the means are well below the values in the standards. The maximum values for the UDI, Seeger and IDEA studies are just slightly above the standard value. These results may be related to the increased use of thick cushions since the 1970s and elevated seating systems that position smaller individuals at a more functional height. The earlier research may not have included people of very small stature.
Figure 8. Eye Height
When the ANSI A117.1 (1980) Standard was developed, there was a true “standard adult manual wheelchair” but that is not the case today. Wheeled mobility technology has changed significantly and it is likely to continue changing. Many new types of devices have appeared on the market, both larger and smaller than the “standard adult wheelchair” of the 1970s and devices are fitted and customized more often to suit the needs of an individual. In the U.S., as the average weight of the population has increased, wheelchair manufacturers started producing wheelchairs with larger capacity and many more seat widths.
To provide realistic guidance for designers, information on wheeled mobility dimensions should include occupied sizes as well as device size and also include accessories as they are used in everyday life. Occupied device sizes are clearly preferable and more useful for designers than unoccupied sizes but it is not uniformly provided in the standards. For example, in the U.S. standards, only occupied length is shown whereas the width is based on the device alone. Unoccupied device size is important also because it defines the absolute bottom line for small clearances, e.g. knee clearances or closet openings. It is important to note that although data on device sizes is available from manufacturers, it does not include actual dimensions as set up for individuals nor does it provide data on added equipment like seating systems, cushions, control boxes, ventilators, carrying baskets and other accessories. In this regard, not all the studies measured unoccupied dimensions or included accessories as part of their dimensions and measurements (e.g. Stait et al., 2000).
Data on occupied device sizes is most valuable for establishing clear floor area requirements. Thus, if occupied sizes are included in standards, it is important that they be consistent with the specified clear floor areas. Data on armrest, seat, and eye heights can be very useful for designers but it also can be misleading if not enough detail is provided. Design for extremes of a range may help only a very few people, yet design for the mean or median may exclude those in the extremes which may be very useful in the design of facilities that large numbers of wheeled mobility users may inhabit on a daily basis. If this data is reported in the standards, it should include enough information and guidance for designers to make informed decisions about how it is to be used.
The inclusion of handle height in the standards is of questionable value. We could not identify any need for this data. On the other hand, it would be useful to have information on accessory dimensions like control boxes and ventilators.
The illustrations used to depict wheeled mobility devices in the U.S. Australian and U.K. Standards are manual wheelchairs. The Canadian standard, however, includes illustrations and data on scooters and power chairs. This information can be very valuable to designers who are seeking to ensure full accessibility beyond minimum required levels. Additional illustrations are needed to convey the diversity in the devices and their occupants. Designers could also benefit from more information on device size to plan spaces like storage areas for wheelchairs at transportation terminals or the design of counter edges in relationship to armrests. For example, the U.K. standard includes data on the width of folded wheelchairs. Accurate and reliable data on device size may be more appropriate to provide in a reference manual with more detailed information and extensive illustrations of different equipment types in use.
Recommendations
- Provide illustrations of seven types of devices in an advisory section: attendant propelled manual chairs, old style manual chairs, lightweight manual chairs, power assisted chairs, power chairs with rear wheel drive, power chairs with mid wheel drive, scooters.
- Provide data on key characteristics of wheelchairs as used by individuals:
- Occupied width
- Occupied length
- Knee height
- Seat height
- Toe height
- Armrest height
- Eye height
- Head height (currently not included in the Guidelines but useful for vehicle design and also locations where lifts are installed that may not have sufficient headroom)
- Weight (currently not included in the Guidelines but critical for designing lift capacity and structural loads for ramps)
- For advisory purposes, provide statistical information on each variable from which percentile data can be calculated:
- Min-max values
- Standard deviation
- Median
- Update criteria that are based on the above dimensions. This includes but is not limited to clear floor areas, shower seat height, toilet height.
4.2 Clear Floor Area
Figure 9 and Table 3 show the standards from the four countries related to clear floor area. Figures 10-13 show the key findings from the research.
Figure 9.
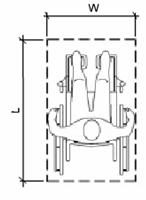
Table 3.
|
|
U.S. |
Australia |
Canada |
U.K. |
|
Width (W) |
760 |
800 |
750 |
900 |
|
Length (L) |
1200 |
1300 |
1200 |
1350 |
Figures 10-11. Clear Floor Area (Occupied) Width for All Devices
Figures 12-13. Clear Floor Area (Occupied) Length for All Devices
Recent revisions to standards in Australia and the U.K. have increased the clear floor area dimensions in both width and length. The U.K. requirements, in particular, are much larger requirements than those in the U.S. and Canada. Research results support larger dimensions. All the studies found that wheeled mobility devices vary from the standards significantly in both width and length. While there are many occupied devices that are narrower and shorter than the values in the standards, the largest devices are generally above the minimum width and length in the standards.
The findings on clear floor area are based on the findings on occupied width and length, where provided. The DETR study did not collect data on occupied width (see previous section). The authors argued that individuals can bring their arms and legs inboard when entering transportation vehicles and passing through doorways. We found, however, that many individuals cannot bring their body parts “inboard”.
The IDEA Center research results for occupied width were smaller than those of the Seeger study. No study reported widths larger than 850 mm. The BS8300 research did not report occupied widths larger than 800 mm but the BS8300 standard, as we interpret it, requires 100 mm more than that for the clear floor area width (900mm). The BS8300 standard’s developers may have added 100mm to provide additional maneuvering room at clear floor areas.
In all the studies that reported data by device type and percentile, the occupied widths of the smallest and largest power chairs were generally the same as the occupied widths of the manual chairs. Occupied widths of scooters were narrower with the exception of the IDEA Center findings. This can be attributed to the presence, in the IDEA scooter sub-sample, of some very large individuals and some who keep their legs outside the edge of the chair when in a resting position. Other studies may not have measured people in “resting” postures. The larger sizes of Americans may also contribute to this difference.
The largest occupied lengths all exceed the current standards, even the U.K. standard of 1350mm. However, the results show that the 95th percentile values are between 1200 and 1350 mm. The difference between the maximum length in the UDI and Seeger studies and the others is so great that it is probably due to the presence of unusually large people and/or devices or measurement error. The maximum length (occupied) recorded in the UDI study, for example, was over 2000 mm (over 6 ft.- 8 in.)! In the case of Seeger et al.’s work, we know that most of the sample was recruited from institutions and many may have had extended foot rests or reclined backs on their chairs. No information is provided in the reports to assess whether individuals in either study could be considered outliers. For example, the other studies together included over 1200 individuals and no other study reported a device as long as 2000 mm. Such a large value is likely to have been a measurement error or a very unusual case such as a person who uses a small all terrain vehicle for mobility.
The research results clearly suggest that clear floor areas be increased to address the actual size of contemporary occupied devices. Although there are differences in the findings, they can be attributed to methods and reporting approaches.
Recommendations
- The clear floor area width should be increased in the U.S. standards. A width of 800 mm (31.5 in.) would accommodate the 95th percentile in the IDEA sample
- The clear floor area length should be increased in the U.S. Standards. A length of 1400 mm (55 in.) would accommodate the 95th percentile in the IDEA sample
4.3 Reach Ranges
Figures 14-15 and Table 4 show the standards from the four countries related to reach from a wheeled mobility device. Figures 16-19 show key findings from the research.
Figures 14-15. Forward and Lateral Reach
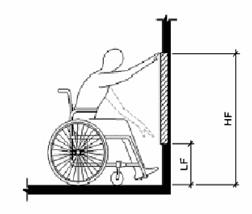
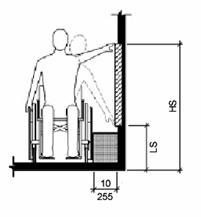
Table 4
|
|
U.S. |
Australia |
Canada |
UK |
|
Unobstructed |
|
|
|
|
|
High Forward Reach (HF) |
1220 |
1220 |
1220 |
x |
|
Low Forward Reach (LF) |
380 |
250 |
380 |
x |
|
High Side Reach (HS) |
1370 |
1350 |
1400 |
1060-1170 |
|
Low Side Reach (LS) |
380 |
230 |
230 |
630-665 |
|
Obstructed |
|
|
|
|
|
High Forward Reach |
1120 |
R.E. |
1100 |
1000-1150 |
|
Low Forward Reach |
x |
x |
x |
650 |
|
High Side Reach |
1220 |
1170 |
1200 |
x |
|
Low Side Reach |
x |
x |
x |
x |
*R.E. = Reach Envelope
The U.S., Canadian and Australian standards are similar, although the latter use a reach envelope to provide guidance for obstructed forward reach and both the Australian and the Canadian standards are less restrictive for low side reach. On the whole, the U.K. standards proscribe much more restrictive reach ranges although they do include different limits for different types of applications.
Figure 16. High Forward Reach
Figure 17. Low Forward Reach
* Three outliers removed from IDEA Center data due to data translation errors in software
Figure 18. Upper Side Reach
Figure 19. Low Side Reach
Note: 3 outliers removed from IDEA Center – Protocol data due to translation errors in software
For the IDEA results, the forward reach graph represents reach over the anterior most (forward) point of the wheelchair or body for trials with no weight lifted (as in Fig. 14-15). We do not know how forward reach was measured in the UDI study. In the BS8300 study, trials were conducted over a counter and it is not known whether the results reported represent highest reach for each person in general or over the anterior most point. It is also not clear who was excluded or included in the UDI and BS8300 results.
The 5th percentile values for high forward reach in both the IDEA and UDI studies are well below the current U.S., Australian and Canadian standard of 1220 mm (48 in.). The reason for the very low 5th percentile and minimum values in the IDEA study is that several individuals’ reach envelope only intersected the anterior most plane at the extended part of their reach envelope (near the bottom of the arch). They could reach higher but only behind the anterior most plane, e.g. if they had knee space in which to pull their device. This may be true of other studies as well but information is not available to understand what is meant by highest reach.
The UDI and IDEA results are remarkably similar given that there are so many ways that reach can be measured. The results indicate that there are some people at the lower tail end of the distributions who have very restrictive reaching ability. The minimum value for the BS8300 research (the only one reported) was close to the current standards. We believe that this is due to either a different measurement technique (highest reach regardless of whether it was behind the anterior most point) or exclusion of individuals in the sample who could not reach to the anterior most point.
High side reach results have a similar pattern although the BS8300 study results were lower than the standards of the other countries. The BS8300 and the UDI results for low side reach were within 100 mm (4 in.) of each other at the minimum end of the range. The participants in the IDEA sample with the most restricted reach ranges were not allowed to reach lower, however, due to the safety considerations imposed.
The reach results for the different studies demonstrate great differences, even though some consistent trends are evident. More information is needed to clarify exactly how the UDI and BS8300 reach studies were completed, how the data in each was analyzed, and who the people with extreme values were. The UDI data may include some outliers that need to be identified and eliminated. The BS8300 study may have excluded people whose reaching ability may be more restricted than those included by the UDI and IDEA center.
The reach results for the different studies demonstrate great differences even though some consistent findings emerged. More information is needed to clarify exactly how the UDI and BS8300 reach studies were completed and how the data in each was analyzed. More detailed information is needed about the people at the extremes in reaching in both studies. The UDI data may include some outliers that need to be identified and eliminated. The BS8300 study may have excluded people whose reaching ability may be more restricted than those included by the UDI and IDEA center. The IDEA Center results demonstrate that some individuals can only reach the anterior or lateral most plane at the extreme of their reach range. Additional analyses, removing individuals whose forward or side reach range is restricted in this way may result in more comparable findings.
Thus, standards should reflect the most functional reaching approach. Besides free reaching ability, there are additional exclusion criteria that could be imposed for the purpose of establishing standards, for example, the ability to lift an object or perform a grasping task. The IDEA Center studied the impact of grasping and lifting a weight during a task. The standards make no mention of the task so those results are not presented here. These data may perhaps be more relevant for developing standards since they are more realistic tasks. Our preliminary analyses of the weighted reach trial data indicate that many of the participants with marginal reaching abilities would be eliminated from an analysis of these trials because they could not perform the task at all (even with the aid of an assistive device called a “cuff” that eliminates the need to grasp the object). The remaining participants are likely to have more extensive reach envelopes and thus the low end of the range could actually be higher than with free reach simply due to exclusion of people with marginal reaching abilities. Our preliminary analysis also indicates that many participants could reach higher at a 45 degree angle than forward or to the side. Thus, this set of trials may provide information for changing the approach used in the standards. Individuals are likely to use the approach that is most functional for them, if there is enough room.
Currently the U.S., Canadian and Australian standards address reach over an obstruction in a very simplistic manner. They specify maximum and minimum heights but do not take into consideration the fact that the depth and height of the obstruction can vary with a corresponding impact on the reach envelope. Reaching over an obstruction was studied in the BS8300 study, and, the limits of obstructed reach can be derived from the IDEA data. But, since there are so many variables that have an effect on reach over obstructions, e.g. knee space depth, armrest height, depth of obstruction, height of obstruction, etc. it is not easy to devise a means to represent it in a way that is useful for designers. The BS8300 approach included different requirements for different scenarios. This seems to offer a promising direction for improving this aspect of accessibility standards.
Recommendations
- Develop revised criteria for reaching from a wheeled mobility device that are more realistic and comparable to everyday tasks.
- Base reach limits on a sample of individuals that excludes those with marginal abilities.
- Advisory information should be used either in the standards themselves or in a companion document to help designers address the variety of reaching conditions not specifically addressed in the requirements. That is the approach that the U.K. has taken in BS8300.
- Examine the implications of knee clearance on reach envelopes.
- Develop a method to represent reaching over obstructions.
4.4 Knee and Toe Clearances
Knee and toe clearances of the four sets of standards are roughly comparable. Figures 20-21 and Tables 5-6 show the standards from the four countries related to knee and toe clearances from a wheeled mobility device. Figures 22-27 show key findings from the research.
Figure 20.
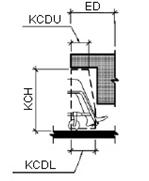
Table 5.
|
|
U.S. |
Australia |
Canada |
U.K. |
|
Knee Clearance Height (KCH) |
685 |
640-650 |
680 |
700 |
|
Knee Clearance Depth (KCDL) |
280 |
230-250 |
200 |
260 3 |
|
Knee Clearance Depth (KCDU) |
205 |
x |
x |
x |
|
Extended Depth (ED) |
635 |
620-640 |
X |
500-650 |
|
Reduction Angle |
1:6 |
X |
X |
X |
|
Width |
760 |
800 |
750 |
900 |
Figure 21.
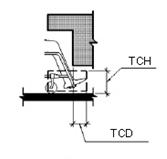
Table 6.
|
|
U.S. |
Australia |
Canada |
U.K. |
|
Toe Clearance Height (TCH) |
230 |
280-290 |
230 |
300 |
|
Toe Clearance Depth (TCD) |
150 |
190-200 |
230 |
X |
|
Width (W) |
760 |
X |
750 |
900 |
Figures 22-23. Knee Clearance Height
Note: DETR (U.K.) values are estimates
* One outlier from IDEA Center data removed because the wrong dimension was originally reported.
Figures 24. Knee Clearance Depth
* Two outliers from IDEA Center data removed due to translation errors in software.
The IDEA and DETR results for knee clearance size are not entirely consistent. But, they demonstrate that current standards generally accommodate the research participants except at the 95th percentile and above. The BS8300 sample had very little variation in knee clearance height. This suggests that the sample may have been much less diverse than the other two samples. A review of photographs of participants in the IDEA sample indicates that the largest individuals are not always the ones who need the greatest knee clearances. Smaller individuals who have heavy thighs, those with high seats and scooter users also have high lap heights. Individuals with extended footrests and scooter users have deep knee clearances. The knee clearance depth required by the U.K. standard is shallower than the others. But, the BS8300 research did not include this variable.
Figure 25-26. Toe Clearance Height
Note: DETR (U.K.) values are estimates
*Two outliers from IDEA Center data removed due to translation errors in software
**One additional outlier from IDEA Center- adjusted data removed due to foot position of one subject (dotted line)
Figure 27. Toe Clearance Depth
* Four outliers from IDEA Center data removed due to data translation errors in software
The IDEA, DETR and BS8300 research are the first to complete a study of knee and toe clearances. The studies are not entirely consistent but taken together, they provide convincing data on the need to make some changes in both knee and toe clearance dimensions. Note that the greatest discrepancy is between the BS8300 data and the other two studies. Again, the BS8300 results suggest that the sample used was not very diverse.
Results from the IDEA and DETR studies indicated that the 80th percentile participants and above are not accommodated by current standards for toe clearance. Again, the largest individuals are not always the ones who require the highest or largest toe clearance. In particular, people with small stature who have elevated seating systems need a very high toe clearance since the entire body becomes elevated. Scooters need a deep toe clearance as we defined it but many scooters have pivoting seats that allow their users to take a side approach to devices and fixtures. People with extended footrests require both deep and high toe clearances.
The IDEA Center data collection methods allowed calculations of lap height as well as knee height. Lap height was used as the determining value for knee clearance. A reanalysis using knee height may result in a closer fit with the DETR data but that does not necessarily mean that knee height should be the controlling variable.
It is clear that those people who need the largest knee and toe clearances cannot be accommodated without making some radical changes to the design of counters, drinking fountains and other design features where knee space is provided. Policy makers have to make a decision about who should be accommodated by knee and toe clearances or require alternatives like providing side access as well as front access. The results clearly provide evidence that adjustable and adaptable counters and toe kicks are a valuable design strategy. They suggest that more emphasis should be placed on adjustability, especially in home environments.
Recommendations
· A policy decision is needed on whom to accommodate for knee and toe clearances. Knee clearance and toe clearance height and depth requirements would have to be raised significantly to accommodate the individuals in the IDEA and DETR sample who need the largest clearances. However, that would result in some serious negative impacts for counter design, drinking fountain design and other design features where knee space is provided.
· Consider requiring both a lateral approach to counter and service desks in public places and a forward approach under the work surface.
· Consider the use of adaptable clearances as a way to accommodate more people when needed.
4.5 Maneuvering Clearances
Figures 28-29 and Tables 7-8 show the standards from the four countries related to maneuvering clearances from a wheeled mobility device. Figures 30-32 show key findings from the research.
Figure 28
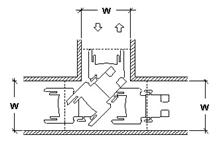
Table 7.
|
|
U.S. |
Australia |
Canada |
U.K. |
|
Width (W) |
915 |
X |
920 |
X |
Figure 29
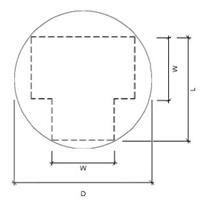
Table 8.
|
|
U.S. |
Australia |
Canada |
U.K. |
|
Diameter (circular) |
1525 |
X |
1500 |
1500 |
|
Width (W) |
X |
1540 |
X |
X |
|
Length (L) |
X |
2070 |
X |
X |
Figure 30. 90 Degree (“L-Turn”) for All Devices
Note: IDEA Center values “max out” at 1000 mm due to experimental protocol
Figure 31-32. “U-Turn” for All Devices
Only the U.S. and Canada have requirements for 90 degree or L-Turn clearances. All the standards have requirements for “wheelchair turning spaces.” Canada includes guidelines for both a 360 degree turn and a 180 degree turn. But, it is not clear, how the different standards define these turns. For example, when should one plan for a 360 degree turn as opposed to a 180 degree turn? Australia defines a rectangular area where the other countries have adopted a circular or “T-turn” geometries. Canada and the U.K. have added informative sections with more advisory information on maneuvering space requirements. This advisory data is based on the research reported in the UDI report and BS8300 Annex respectively.
The clearance required for all participants to complete a 90 degree turn by the IDEA sample was much smaller than the UDI findings. An increase in the clear width criterion of 100 mm (4 in.) would be needed to accommodate the entire IDEA sample. However, to accommodate the entire UDI sample, an increase of 300 mm (12 in.) would be needed. The UDI findings at the high end of the range probably reflect the impact of a few participants or devices with very poor turning ability.
The IDEA protocol included only a 360 degree turn but the UDI study included a 180 degree turn as well. The BS8300 reports only the latter but doesn’t define it. The IDEA and BS8300 results demonstrated that turning area clearances would have to be increased to 2400 mm (94.5 in.) compared to the current 1500-1525 mm (60 in.) to accommodate their entire samples. To accommodate the UDI sample for a 180 degree turn, the required turning space would only have to be increased to 1925 mm (75.8 in.). However, in the UDI research protocol, the ends of the turn were open, allowing the participants to lengthen out their turn and reduce its width. In comparison, the UDI participants utilized a much larger space for the 360 degree turn, in which no sides were blocked. A space about 4200 mm (165 in.) would be needed to accommodate the entire sample. In the IDEA sample, scooters require more space but the largest values for scooters, power chairs and manual chairs were very close whereas in the UDI sample, at least one power wheelchair user required a much larger clearance for the 360 degree turn. Because the UDI protocol for the 360 degree turn was not bounded by walls, participants could extend their arms and legs beyond the envelope of the chair. With a bounded area, many of these individuals may have been able to pull their extremities closer to their body during the turn.
The results support increasing the clearances for 90 degree turns and 180 degree turns. However, it appears that there are some people at the tail of the distribution who require much larger spaces than even the 95th percentile values. More detailed information on who these individuals are and the size of their devices is needed. They may be very restricted in their abilities to maneuver chairs independently. It is important to note that these individuals use all three types of devices. We observed some manual wheelchair users who had very restricted push arcs. This limited their ability to maneuver a chair and resulted in wide turning circles.
The differences between the UDI findings and the other studies suggest great differences in their protocol or measurement technique. This may be due to the lack of an enclosure in the 360 degree turn, errors in correcting for parallax when measuring from video cameras mounted above, or inability to obtain accurate measurements of body parts and devices in motion.
Recommendations
- Clearances for L-turns should be increased 100 mm (4 in.).
- The intent and applications of the wheelchair turning area needs to be more clearly defined.
- Clearances for wheeled mobility device turns should be increased but accommodating the entire population of wheeled mobility users may result in very restrictive requirements.
User Comments/Questions
Add Comment/Question