Best Practices in the Design of Toileting and Bathing Facilities for Assisted Transfers
Design Specifications
Water Closets (ADAAG 4.16)
4.16.2 Clear Floor Space.
In order to accommodate independent wheelchair use, guidelines for clear floor space in ADAAG vary according to path of approach to the toilet. However, in accommodating assisted transfers, these guidelines were less of an issue than providing space adjacent to the water closet for caregivers and including a 5’ turning radius in the room for wheelchair maneuvering. As a result, toilet room configuration and location of the water closet were the critical design considerations in assisted transfers.
Toilet Room Configuration.
The most common practice among the innovative designs was the placement of the bathroom located in a corner of a resident room with an out-swinging bathroom door oriented at 450 to the resident room. The 450 angle facilitated maneuvering by eliminating the need for sharp turns in small spaces. In addition, the location of the door also permitted the toilet and lavatory in many facilities to be located at right angles to each other. This configuration provided room for a 5’ wheelchair turning radius as well as sufficient room for assistance on both sides of the toilet. Furthermore, the out-swinging door not only permitted a 5’ turning radius in the toilet room, but also facilitated entry by staff in the event of a resident fall or other incapacity inside the room that might block the door. This basic configuration was found in numerous facilities including: a nursing care addition at Pennswood Village Retirement Community, Newton, PA (Lewis and Rodgers Architects, Fort Washington, PA) (Figure 1); Bridges Medical Services, Ada, MN (Horty, Elving & Associates, Inc., Minneapolis, MN) (Figure 2); and The Heritage at Landis Homes Retirement Community, Lititz, PA, (RLPS) (Figure 3).

sd
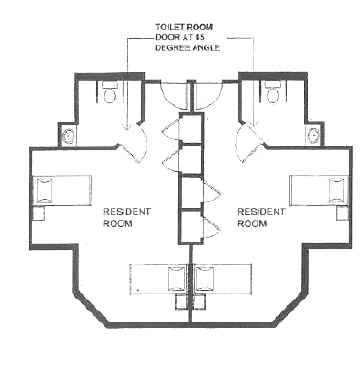
Figure 2. Toilet Room Configuration at Bridges Medical Services, Ada, MN (Horty, Elving & Associates)

Figure 3. Toilet Room Configuration at The Heritage at Landis Homes Retirement Community, Lititz, PA(RLPS)
Water Closet Location.
In contrast to ADAAG, which specifies that the centerline of the toilet shall be located 18" from a sidewall, every innovative design located the toilet further away from the sidewall in order to provide space for caregivers to stand alongside one or both sides of the toilet. However, without research data upon which to determine how much space was adequate, side clearance varied, usually dependent on the amount of space available within the overall design of the room or facility. Although 24" seemed to be the norm, the location of the toilet ranged from as little as 22" to as much as 30" from the sidewall.
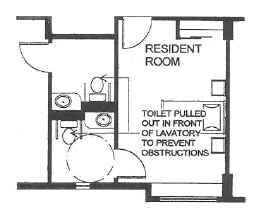
For example, at two skilled nursing facilities, one for people with Multiple Sclerosis, Cerebral Palsy, and spinal cord injuires (Beechwood Home, Cincinnati, OH) and one for frail older adults (The Ledges at Rockynol, Akron, OH), Dorsky Hodgson and Partners located the toilet with the centerline 24" from the closest sidewall. In addition, at Beechwood Home where the lavatory was located adjacent to the toilet on the opposite side, the rear wall behind the toilet was pulled out so that the back of the toilet was not in the same plane as the lavatory. This effectively pulled the toilet out in front of the lavatory, thus preventing the latter from interfering with assistance on that side of the toilet (Figure 4).
Figure 4. Water Closet Location at Beechwood Home (Dorsky Hodgson and Partners)
In contrast, at Covenant Oaks at Oakwood Village, a dementia-specific assisted living facility in Madison, WI, OWP&P was only able to provide 22" from the sidewall to the centerline of the toilet (Figure 5). Although more space was preferable, it was not available in this facility. Nonetheless, this deviation from ADAAG as well as Wisconsin’s accessibility code was requested by the owner to facilitate assisted transfers and required a variance from the City of Madison.
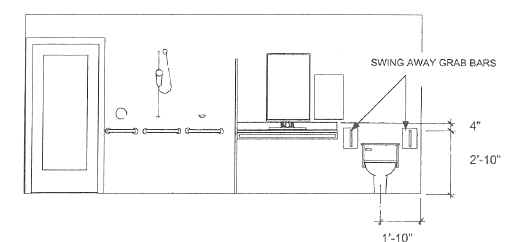
Figure 5. Water Closet Location at Covenant Oaks at Oakwood Village, Madison, WI (OWP&P)
The general sentiment among designers was that more space was better. As a result, a number of projects (Figures 6-8) were designed to provide more than 24" of space for assisted transfer. In facilities designed by Nelson Tremain Partnership, 30" between the wall and toilet was the design goal. However, due to space limitations, that goal is difficult to achieve. At Creekview at Evergreen Retirement Community in Oshkosh, WI, 26" was available (Figure 6), while at Village Shalom, a nursing home in Overland Park, KS, only 24" was available (Figure 7). Twenty-four inches between the side wall and toilet was fairly common. For example, at Memorial Hospital of Martinsville and Henry County (Martinsville, VA), Ellerbe Becket provided 24" between the wall and the side of the toilet on each side at the request of nursing staff at the facility (Figure 8). Staff felt that 24" would provide sufficient space for them to fit on both sides of the toilet and still permit a patient to reach the wall-mounted toilet paper holder without falling off the toilet.
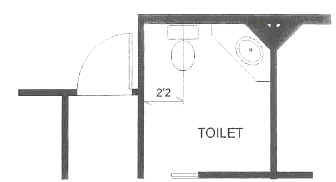
Figure 6. Water Closet Location atCreekview at Evergreen Retirement Community, Oshkosh, WI (Nelson Tremain Partnership)
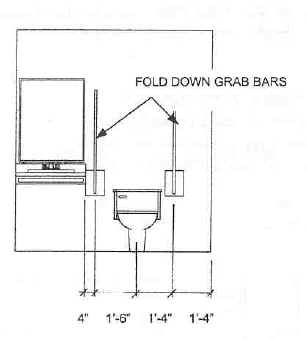
Figure 7. Water Closet Location atVillage Shalom, Overland Park, KS (Nelson Tremain Pertnership)
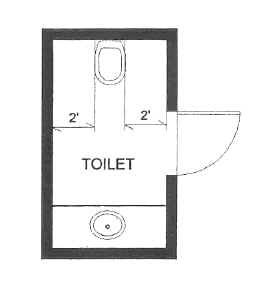
Figure 8. Water Closet Location at Memorial Hospital, Martinsville, VA (Ellerbe Becket)
The most unique concept was that of a "training toilet" developed by OWP&P based on the European model of "bathroom as shower room." Ostensibly, the idea of the training toilet was to circumvent the limitations of accessibility requirements, by designing bathroom facilities that were intended for training residents rather than for their actual use. Training toilets were either located in a separate room as a unisex toilet or combined with a bathing facility, for use by staff in retraining residents in toileting skills. Typically, these designs included swing away grab bars on both sides of the water closet and up to 3 feet of clearance on either side. As a result, the floor area needed for a "training toilet" was substantially more than for a conventional ADA-compliant toilet room. When this configuration was used at the Memory Loss Unit, a dementia care assisted living facility at C.C. Young Retirement Community in Dallas, TX (Figure 9), it was challenged by both the Dallas Building Department as well as the reviewer for compliance with the Texas Accessibility Standards (TAS). Approval was granted when it was demonstrated that other readily available toilet rooms complying with ADAAG and TAS were provided.
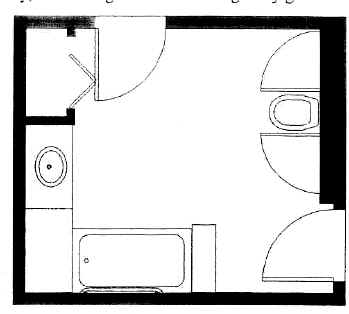
Figure 9. Water Closet Location at Memory Loss Unit at C.C. Young Retirement Community, Dallas, TX
4.16.3 Height.
All of the institutional designs included a raised toilet within the 17"-19" range allowed by ADAAG. Although the seat height did not differ from ADAAG specifications, the reasons for a higher seat did differ. Whereas the rationale for seat height in ADAAG is to provide a surface that is at or slightly below the wheelchair seat in order to accommodate a sliding transfer, the rationale in eldercare facilities was to minimize the distance individuals had to be lowered down or raised up. It is important to note that although designers knew that a higher seat was necessary, there was no data to suggest what the optimal seat height might be. In the absence of data, the 17"-19" range for seat height was selected to comply with ADAAG.
4.16.4 Grab Bars.
Among the various specifications for grab bars in general, including diameter, spacing, and structural strength (ADAAG 4.26) and for toilets in particular, including length and positioning, only the latter two were adjusted to accommodate assisted transfers.
Positioning. According to ADAAG, positioning is dependent on two factors, height and location of grab bars, both of which were altered by designers to better accommodate an older population.
Height. Only two firms, OWP&P and Nelson Tremain Partnership specifically addressed the issue of height. OWP&P used the high end of ADAAG (33") whereas Nelson Tremain used 10" above the seat height. Although OWP&P did not deviate from ADAAG, the intent was to account for the reduced stature of many older adults as well as to optimize their potential leverage. The maximum height in ADAAG was used because there was no other objective information available upon which to base a decision on effective height for assisted transfers.
In contrast, Nelson Tremain, in the absence of objective data, rationalized that height of toilet grab bars be based on the distance between the seat and arms of a chair. Thus, they decided to locate the bars 10" above the height of the toilet seat, whereas ADAAG permits grab bars 14"-19" above the seat. Although there is no evidence to support this rationale, common sense suggests that lower grab bars would enable caregivers to lean over the bars to provide assistance as well as permit individuals to be able to push up more effectively from the toilet.
Location. The ADAAG L-shaped grab bar configuration that includes a bar on the sidewall and one on the rear wall behind the toilet was consistently considered inadequate to meet the needs of people requiring assistance. As Gregory Scott, AIA, partner in RLPS, responded:
"…the major challenge with the implementation of ADAAG, is not with excessive space requirements or even required clearances; but more with achieving non-institutional appearances and being required to install assistive devices, such as wall-mounted grab bars at toilets, that serve no useful purpose for our age group [persons 78+ years of age]. We often end up installing redundant grab bars; one set to meet guidelines, the other set to meet the true needs of the resident. We are discovering that grab bars mounted at the recommended heights and distances from the toilet, both side and rear locations , are too far away to be effective for ‘self’ assistance. The seat mounted grab rail or fold-away models can place the ‘assistance’ where it is useful."
Subsequently, the rear grab bar behind the toilet was omitted in all configurations intended to accommodate assisted transfer. Similarly, the sidewall grab bar was often omitted. When this grab bar was used (e.g. Memorial Hospital of Iowa County, Dodgeville, WI, Nelson Tremain Partnership), it was intended to be used as a support for a standing individual during dressing and a swing away grab bar was provided on the opposite side of the toilet (Figure 10).
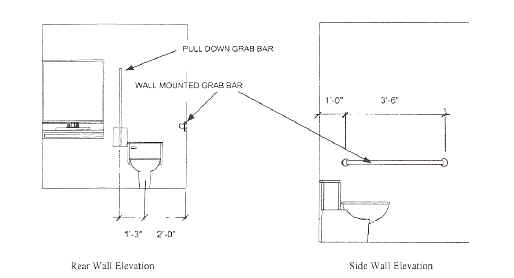
Figure 10. Grab Bar Location at Memorial Hospital of Iowa County, Dodgeville, WI (Nelson Tremain Partnership)

Figure 11. Location of Swing Away Grab Bars (Linido grab bars pictured here)
Rear-mounted (either floor or wall), swing away (or fold up) grab bars (e.g., Linido or Bobrick) on both sides of the toilet were the most popular configuration to accommodate one or two person-assisted transfers as well as independent toileting (Figure 11). Those designs that did not utilize these grab bars either used straddle bars (non-movable) that flanked both sides or simply applied ADAAG for compliance purposes and then added additional grab bars to meet the needs of the clients. Rob Pfauth, AIA, a design architect at OWP&P stated that:
"grab bars on both sides of water closets that either swing up or away obviously afford the ability for one or more caregivers to stand beside the resident and brace them while mounting or dismounting the toilet. Yet these grab bars, when in the extended position alongside the water closet provide superior leverage to the frail older adult, dependent on his or her waning upper body strength, in lowering or lifting themselves during independent toileting. Installing grab bars on both sides is important, particularly for stroke victims with hemiplegia, as a conventional sidewall grab bar on the "wrong" side is virtually useless for transferring."
Length. Whereas none of the respondents specifically addressed the issue of grab bar length, drawings submitted clearly indicate that many of the alternate swing away grab bars were considerably shorter (usually 24"-30") than the 42" minimum requirement for grab bars alongside the toilet (Figure 12). As these bars were used by individuals who often had unsteady gait and were at risk of falls, the shorter bars were likely to have been used to enable both older individuals and caregivers to get as close to the toilet as possible and thereby minimize ambulation.
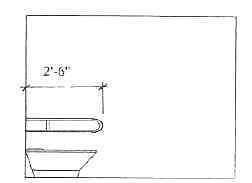
Figure 12. Length of Grab Bars
4.16.5 Flush Controls.
None of the respondents indicated that there were any variations from ADAAG regarding flush controls.
4.16.6 Dispensers.
Few of the respondents specifically addressed the issue of dispensers, even though increasing the distance between the sidewall and the toilet would suggest that locating dispensers on the sidewall within 18" of the centerline of the toilet (as specified in ADAAG) was not possible. However, Roland Binker of Ellerbe Becket, indicated that nursing staff at Memorial Hospital of Martinsville and Henry County (Martinsville, VA), felt that 24" would provide sufficient space for staff and still permit a patient to reach a wall-mounted toilet paper holder without falling off the toilet. Alternatively, Horty Elving and Associates used a toilet paper holder at the end of each swing-away grab bar (e.g., Figure 11) at Bridges Medical Services, Ada, MN (Horty, Elving & Associates, Inc.), a facility that received a Best in Category by Design ‘99 Awards sponsored by the AIA and AAHSA. A second alternative, used at Creekview at Evergreen by Tremain Nelson Partnership, was to locate a dispenser for caregiver, rather than for user convenience. As a result, the dispenser was located 24" above the floor, 5" higher than the minimum height in ADAAG, and 42" from the rear wall (Figure 13), which would have been too high and too far in front of most older users for them to reach safely.
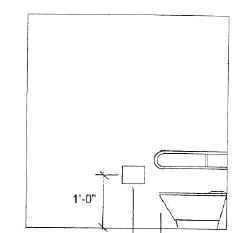
Figure 13. Location of Dispenser at Creekview at Evergreen, Oshkosh, WI (Nelson Tremain Partnership)
Bathtubs (ADAAG 4.20)
ADA Accessibility Guidelines for bathtubs are predicated on the use of a conventional residential bathtub by individuals who independently transfer from a wheelchair directly to a tub seat. However, most eldercare facilities used larger whirlpool baths not conventional residential tubs. Moreover, frail older adults usually have the ability to stand. Therefore they are more likely to transfer into the tub from a standing position regardless of whether they used a wheelchair, walking aid, or no aid at all. Nonetheless, because stepping over the side of the tub as well as lowering down and raising up from the bottom of the tub is a potential safety risk for these individuals, designs were based on caregivers providing assistance and supervision during transfers and bathing. Resident lifts, which are an alternative means of safely transferring an individual into a tub, were generally discouraged, particularly among people with dementia because the experience of being lifted off the ground and lowered into a tub can be a terrifying one for them. However, for more acute populations including a lift was sometimes unavoidable.
4.20.2 Floor Space.
The amount of clear floor space in front of a bathtub required by ADAAG (30"-48" min depth depending on the direction of travel by the length of the tub including a seat at the head of the tub) is based on positioning a wheelchair along side the fixture for a sliding transfer. However, because frail older adults do not perform sliding transfers, clear floor space in eldercare facilities was needed for one or more caregivers to be able to assist with getting in and out of a tub. This not only affected the size of the space, but also where the space was needed.
Therefore, residential tubs that are only accessed from one open side, were typically designed with one end against a wall and 3 open sides from which assistance could be provided. Because wheelchair maneuverability was not an issue, less space was needed on any one side. However, more space was needed overall to accommodate caregiver access from more than one side.
4.20.3 Seat.
As tub seats are intended to keep users from being immersed, the use of tub seats defeated the purpose of providing a whirlpool bath. As a result, tub seats were not provided in conventional whirlpool bathtubs, although they were used in walk-in fixtures (see Alternative Designs below).
4.20.4 Grab Bars.
ADAAG specifications for grab bars vary slightly for bathtubs with in-tub and head of tub seats (the latter having longer bars on the sidewall and no bar on the head wall). Nonetheless, in both conditions, grab bars are located to help individuals get into the tub and then to lower and raise themselves to and from a seated position. Because these positional changes were deemed safety risks for older adults, grab bars that would permit older adults to raise and lower themselves were not included in most bathtub designs (see Alternative Designs below). Rather, in most designs, grab bars were provided adjacent to the tub for temporary support to enable an individual to steady him/herself while a care provider assisted with removal and replacement of clothing. In fact, in instances where local building authorities required bathing fixtures with ADAAG compliant grab bar configurations, roll-in showers were installed instead due to safety concerns, even though the former were readily available from a number of manufacturers.
4.20.5 Controls.
None of the respondents indicated that there were any variations from ADAAG regarding controls.
4.20.6 Shower Unit.
None of the respondents indicated that there were any variations from ADAAG regarding the shower unit.
4.20.7 Bathtub Enclosures.
None of the respondents indicated that there were any variations from ADAAG regarding the enclosure except for the walk-in fixture described below.
Alternative Designs.
One alternative design that was used by OWP&P for less frail, ambulatory individuals was the Kohler "Precedence" bathtub (Figure 14). The tub has a non-institutional appearance, a fold-down seat, and a swinging side entry door with a pressurized seal for ease of access. Similar "walk-in" units, although slightly more institutional in appearance, are made by Arjo ("Freedom" tub) and others. The walk-in capability makes this fixture suitable for either independent or assisted use by individuals with a reasonable level of mobility. In addition, the fixture is also taller than most average bathtubs (24" above the finished floor) which permits immersion in the water even when using its fold-down seat. Whereas the added height and side-entry features address the primary shortcomings of a traditional tub, they also create the two shortcomings of this tub. First, it must be drained to open the door to exit the fixture. As a result, an older individual who can only get out through the door must sit in the tub until it is drained. Second, the tub does not meet ADAAG grab bar provisions. The 24" high sides make it impossible to install the two grab bars on the back wall in the manner prescribed in ADAAG. As a result, in facilities where this fixture (Figure 15) was used, one of the back wall bars was eliminated in order to comply with the distance of 9" from the rim of the tub and 33" –36" distance from the floor to the grab bar. In addition, OWP&P placed a low wall surrounding the tub on one or more sides (usually the foot end and/or the long side opposite the entry). Although this increased the overall space requirement for the bathing room, it provided easier access by a caregiver to assist in the bathing process, enabling them to sit on the wall as well as reach over it.

Figure 14. KohlerPrecedence Bathtub
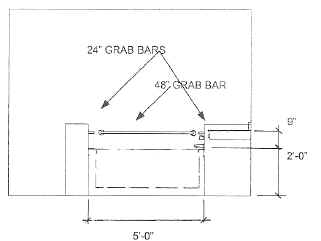
Figure 15. Bathtub Configuration at Memory Loss Unit at C.C. Young Retirement Community, Dallas, TX (OWP&P)
Shower Stalls (ADAAG 4.21)
Although ADAAG permits both transfer and a roll-in showers, roll-in showers were found in institutional facilities. As a result, design of shower stalls was intended to accommodate caregiver assistance with washing, rather than assistance with transfer into the fixture.
4.21.2 Size and Clearances.
Minimum guidelines for roll-in shower stalls are based on residential size fixtures (30" x 60" minimum or the space used by a standard residential tub/shower unit) and spaces (30" minimum depth by the length of the shower, but not less than 48"). Institutional showers exceeded the minimum stall dimensions. However, because users were not expected to independently maneuver their wheelchairs, the critical issues regarding floor space both outside and inside the shower were the amount of space available for caregivers to provide assistance. Outside, the shower space was needed for one or more caregivers to help an individual who needed a shower chair to get into and out the chair. Inside the shower, space was needed to provide assistance with showering without getting wet. To this end, several projects incorporated a half height wall to enable a caregiver using a hand held shower to stay dry while standing behind a resident seated in a shower chair.
4.21.3 Seat.
Seats are only required in transfer showers, which were not used in any of the designs reviewed. When seats were used in roll-in showers, built-in shower seats were typically omitted in favor of movable shower chairs or benches to provide more room and flexibility in accommodating people who required different levels of assistance.
4.21.4 Grab Bars.
ADAAG specifies grab bars on the three walls of a roll-in shower stall, 33"-36" above the floor. The plans reviewed offered little insight as to placement of grab bars in showers. In fact, information about grab bars tended to be contradictory. On the one hand, transfers are typically only made into shower chairs outside the shower and with a caregiver’s assistance. As a result, grab bars in the shower may not be necessary and their placements can be a deterrent to the required maneuvering room needed by caregivers. On the other hand, grab bars provided according to ADAAG are insufficient for independent use of the shower. As a result, more bars, particularly vertical ones, and in different configurations than specified in ADAAG were often installed. However, the location and orientation of grab bars were dependent on the type and size of shower provided.
4.21.5 Controls.
None of the respondents indicated that there were any variations from ADAAG regarding the controls.
4.20.6 Shower Unit.
None of the respondents indicated that there were any variations from ADAAG regarding the shower unit.
4.21.7 Curbs.
All of the designs reviewed were curbless, roll-in showers.
4.21.8 Shower Enclosures.
None of the respondents indicated that there were any variations from ADAAG regarding the shower enclosure.
Alternative Designs. Bathroom as Shower Room.
The bathroom-as-shower-room is a concept adapted from the common European residential model by OWP&P as an alternative for including a shower in every resident bathroom. Due to space constraints at the Oakwood facility (Figure 16), a separate shower stall could not be accommodated in each resident toilet room. Having a shower close to the resident room was particularly important in this dementia facility to allow for impromptu clean-ups in the event of incontinent episodes without the indignity of leading residents down a corridor to a central bathing facility. As a result, each resident bathroom was designed as a shower room that permitted either independent or assisted showering. The latter is facilitated by use of a hand-held shower wand, which can be manipulated by the caregiver standing outside the area enclosed by the shower curtain. Given that this is a dementia care unit, there was a concern that residents might inadvertently douse themselves when left unattended. Thus, care providers can remove shower hoses and wands by a quick-release coupling at the outlet. When this feature was specified, it was expected that it would also cut off the flow of water even if the valve were to be opened. This turned out not to be the case, and a retrofit with an after-market in-line valve installed on the upstream side of the coupling turned out to be impractical due to the danger of backflow.
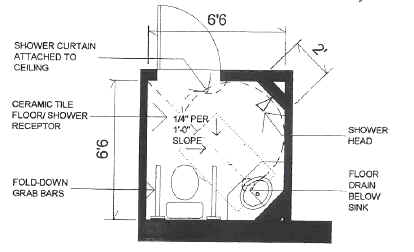
Figure 16. Shower Configuration at Covenant Oaks at Oakwood Village, Madison, WI (OWP&P)
The bathroom-as-shower design requires more space than a typical toilet room as well as special considerations for drainage, doorway design, and waterproofing of other fixtures in the space. However, it affords an enhanced opportunity for assisted showering without the caregiver getting drenched in the process as well as permitting individuals to shower independently.
User Comments/Questions
Add Comment/Question